INTEGRATIVE ARTICLE Open Access
Israel’s rapid rollout of vaccinations for
COVID-19
Bruce Rosen
1,2*
, Ruth Waitzberg
1,3
and Avi Israeli
4,5
Abstract
As of the end of 2020, the State of Israel, with a population of 9.3 million, had administered more COVID-19 vaccine
doses than all countries aside from China, the US, and the UK. Moreover, Israel had administered almost 11.0 doses
per 100 population, while the next highest rates were 3.5 (in Bahrain) and 1.4 (in the United Kingdom). All other
countries had administered less than 1 dose per 100 population.
While Israel’s rollout of COVID-19 vaccinations was not problem-free, its initial phase had clearly been rapid and
effective. A large number of factors contributed to this early success, and they can be divided into three major
groups.
The first group of factors consists of long-standing characteristics of Israel which are extrinsic to health care. They
include: Israel’s small size (in terms of both area and population), a relatively young population, relatively warm
weather in December 2020, a centralized national system of government, and well-developed infrastructure for
implementing prompt responses to large-scale national emergencies.
The second group of factors are also long-standing, but they are health-system specific. They include: the
organizational, IT and logistical capacities of Israel’s community-based health care providers, the availability of a
cadre of well-trained, salaried, community-based nurses who are directly employed by those providers, a tradition
of effective cooperation between government, health plans, hospitals, and emergency care providers –particularly
during national emergencies; and support tools and decisionmaking frameworks to support vaccination campaigns.
The third group consists of factors that are more recent and are specific to the COVID-19 vaccination effort. They
include: the mobilization of special government funding for vaccine purchase and distribution, timely contracting
for a large amount of vaccines relative to Israel’s population, the use of simple, clear and easily implementable
criteria for determining who had priority for receiving vaccines in the early phases of the distribution process, a
creative technical response that addressed the demanding cold storage requirements of the Pfizer-BioNTech
COVID-19 vaccine, and well-tailored outreach efforts to encourage Israelis to sign up for vaccinations and then
show up to get vaccinated.
While many of these facilitating factors are not unique to Israel, part of what made the Israeli rollout successful was
its combination of facilitating factors (as opposed to each factor being unique separately) and the synergies it
created among them. Moreover, some high-income countries (including the US, the UK, and Canada) are lacking
several of these facilitating factors, apparently contributing to the slower pace of the rollout in those countries.
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.
1
Myers-JDC-Brookdale Institute, Jerusalem, Israel
2
Hebrew University Paul Baerwald School of Social Work and Social Welfare,
Jerusalem, Israel
Full list of author information is available at the end of the article
Rosen et al. Israel Journal of Health Policy Research (2021) 10:6
https://doi.org/10.1186/s13584-021-00440-6

Introduction
Worldwide, the year 2020 was dominated by the health
and economic harm caused by the COVID-19 pandemic.
That year ended with a glimmer of hope, as regulators
began to approve COVID-19 vaccines and governments
around the world began to administer them.
Table 1presents data, by country, from the Our World
in Data website [1] regarding the total number of doses
administered and the number of doses administered per
100 population, as of the end of 2020. The table high-
lights two striking things about the State of Israel, whose
end-of-year population was 9.3 million [2]. First, only
three other countries (the US, China, and the UK) had
administered more doses than Israel’s approximately
950,000. Second, Israel had administered almost 11.0
doses per 100 population, while the next highest rates
were 3.5 (in Bahrain) and 1.4 (in the United Kingdom).
All other countries had administered less than 1 dose
per 100 population. As of the end of 2020, Israel’s roll-
out of COVID-19 vaccinations had clearly been rapid
and effective.
As with any major accomplishment, a large number of
factors contributed to Israel’s successful early rollout.
This article begins with a brief overview of the Israeli
rollout, and then discusses 12 factors that contributed to
its early success, with the analysis focusing on the period
until the end of 2020. The concluding remarks note lim-
itations of the analysis and identify several avenues for
further research.
Overview of the Israeli rollout
Israel launched its COVID-19 vaccination campaign on
December 20th, but preparations for it began months
earlier. Over the course of 2020, Israel signed vaccine
purchase contracts with several pharmaceutical compan-
ies at the forefront of COVID-19 vaccine development.
By the time the US FDA had issued an emergency use
authorization for the Pfizer-BioNTech COVID-19 vac-
cine
1
on December 11, Israel already had contracts in
place with Pfizer to purchase and receive a substantial
(but undisclosed) number of doses of that vaccine by the
end of December. Within days, and largely on the basis
of the FDA authorization process, Israel’s Ministry of
Health (MOH) followed with an authorization of its
own.
23
Israel’s MOH also determined (on December 16) that
the initial target groups for vaccination would be people
aged 60 and over, nursing home residents, other people
at high risk due to serious medical conditions, and
front-line health care workers [3]. The responsibility for
vaccinating each of these groups was also clearly defined
at that time:
The primary responsibility for vaccinating the
general population over age 60 and at-risk persons
due to pre-existing medical conditions was assigned
to Israel’s four competing non-profit health plans
Responsibility for vaccinating nursing home
residents was assigned primarily to Israel’s national
medical emergency services organization - Magen
David Adom (MDA).
Responsibility for vaccinating front-line health
workers was assigned to the hospitals and health
plans with whom they work
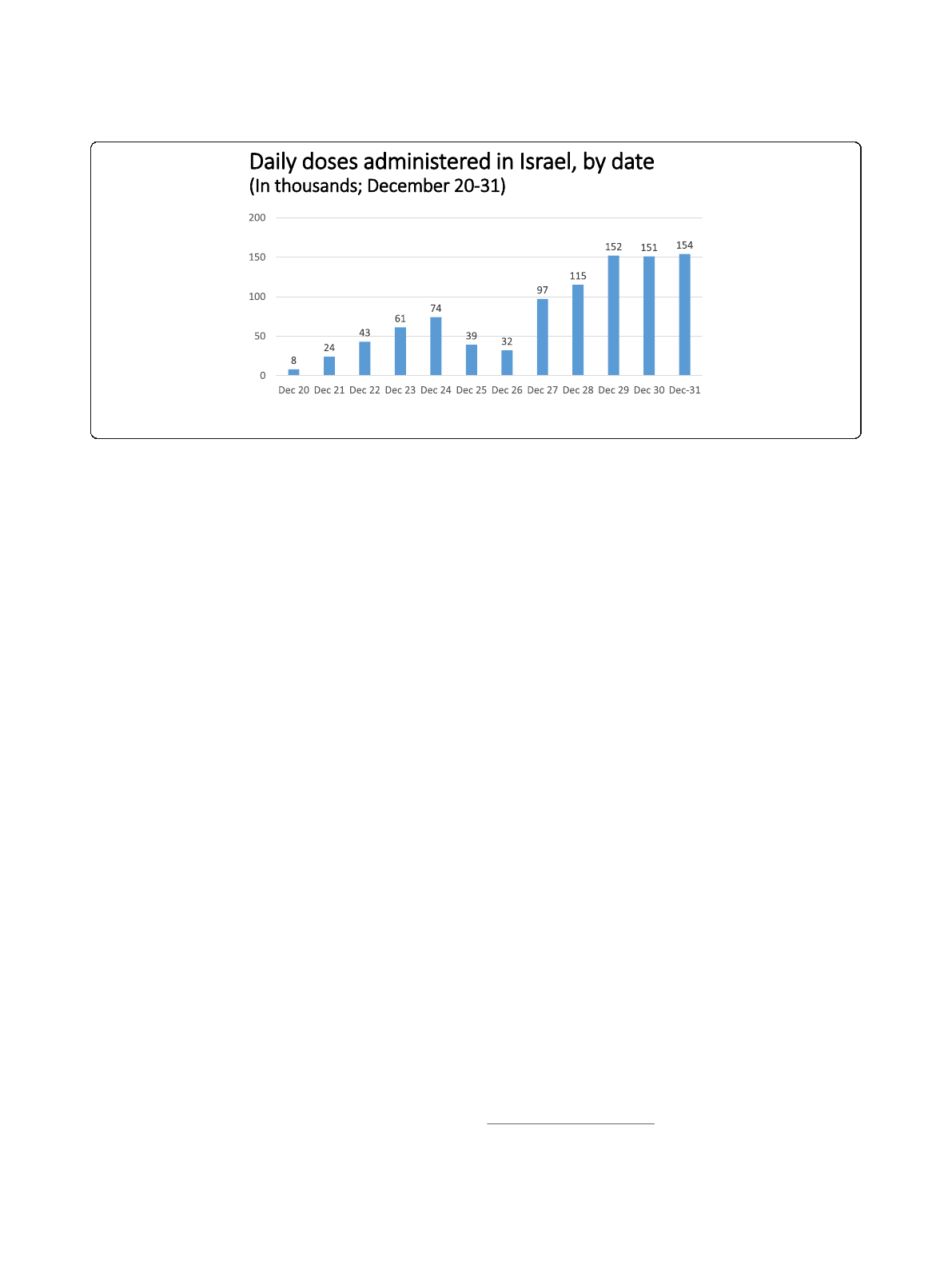
As indicated in Fig. 1, the number of people vacci-
nated per day began at approximately 8000 on Decem-
ber 20, quickly rose to over 70,000 by December 24,
decreased over the following weekend, and then rose to
over 150,000 by December 29.
4
All of the vaccines ad-
ministered in Israel during 2020 were those manufac-
tured by Pfizer, and the vast majority of vaccines were
administered by nurses.
Table 1 COVID-19 Vaccine Doses Administered as of the End of
2020
Listing the 10 countries reporting the most doses administered
Total Doses per Reporting
Country Doses 100 pop’n date
China 4,500,000 0.31 31-Dec
United States 2,794,588 0.84 30-Dec
United Kingdom 963,208 1.42 27-Dec
Israel 949,112 10.97 31-Dec
Germany 165,575 0.20 31-Dec
Canada 99,946 0.26 31-Dec
Bahrain 58,643 3.45 31-Dec
Russia 52,000 0.04 22-Dec
Poland 47,600 0.13 31-Dec
Mexico 24,998 0.02 30-Dec
Source: Our World in Data. https://ourworldindata.org/covid-vaccinations
Note: For each country, the table presents data for the latest date in
December for which data were available in the database
1
The formal name of the vaccine is: Pfizer-BioNTech COVID-19 vac-
cine, BNT162b2 (brand name “Comirnaty”)
2
Personal communication, Boaz Lev, January 2021.
3
At this stage, the vaccine has been authorized for use by people aged
16 and over. There is no prohibition against vaccinating a pregnant
woman or a woman planning a pregnancy. A person with an acute
illness, including a fever of 38 degrees Celsius or above, will not be
vaccinated until they have recovered from that illness. According to
current guidelines, the following are not authorized to receive the
vaccine: people under age 16, people with a history of severe allergic
reaction (who should contact the warehouse nurse to find out if they
can be vaccinated), and people who were confirmed as having been ill
with COVID-19.
4
Israel did not face the issue, present in some other countries, of large
numbers of healthcare workers being on vacation during the week
between Christmas and New Year’s Day.
Rosen et al. Israel Journal of Health Policy Research (2021) 10:6 Page 2 of 14
At the same time, not all was well with the COVID-19
situation in Israel in December 2020, Israel –like many
other countries –was experiencing a major increase in
COVID-19 infections [4], including substantial morbid-
ity among health care professionals. Thus, the vaccin-
ation campaign was launched at a very challenging time
for Israeli health care.
In addition, the vaccination campaign experienced
labor pains of its own. During the first few days of
the rollout, it was quite difficult to schedule an ap-
pointment via the health plans’call centers or digital
tools. In some vaccination sites, not enough people in
the target population showed up, and at the end of
each day vaccines about to pass their expiration time
had to be either thrown away or given to people not
meeting criteria for first-round vaccinations. Even
earlier in the day, some hospitals, health plans and
other vaccine providers were somewhat lax about lim-
iting vaccines to people meeting the official criteria,
thereby increasing the total number of people vacci-
nated, but reducing the supply of vaccines available
to the elderly and other at-risk groups. At some vac-
cination sites, family of health professionals and
members of influential unions or occupations, were
vaccinated even though they did not meet the criteria.
And, while vaccination sites were set up throughout
the country, including in the peripheral regions and
in smaller villages and towns, the rate of vaccine up-
take was markedly lower than average in Arab
localities.
Moreover, as of December 2020 there were many
uncertainties looking forward. There was lack of clar-
ity about when the next vaccine shipments would ar-
rive and how large they would be [5], leading to talk
about a possible temporary suspension of first vacci-
nations (though Israel has been careful to set aside a
second dose for all Israelis and foreign workers
5
who
received a first dose). It was also not clear what pro-
portion of Israelis would ultimately sign-up for vacci-
nations, either due to general anti-Vax sentiments or
to vaccine hesitancy specific to the new COVID-19
vaccines. In addition, it was not clear how the need
to allocate nurses to the vaccination effort was affect-
ing the delivery of other health services. And, as was
the case worldwide, there continued to be uncertain-
ties about how long the vaccine-conferred immunity
would last, how effective it would be against new var-
iants of the virus, and the extent to which it prevents
transmission.
Still, there is no denying that, as of the end of 2020, Is-
rael’s vaccination campaign had achieved a great deal –
both in absolute terms and relative to other countries.
Accordingly, despite its imperfections, and despite the
uncertainties regarding how things would evolve in
2021, it is important to identify and analyze the factors
that contributed to the success of Israel’s vaccine rollout
in its initial phase.
Selected factors contributing to Israel’s success
The specific factors contributing to Israel’s successful
early rollout include, but are not limited to, the
following:
1. Israel’s small size, in terms of both area and
population, its relatively young population, and its
relatively warm weather in December 2020
2. Israel’s centralized national system of government
(as opposed to a federal system of government)
Fig. 1 Daily doses administered in Israel, by date (In thousands; December 20–31). Source: Our World in
Data. https://ourworldindata.org/covid-vaccinations
5
Foreign workers carrying for frail elderly living at home or in nursing
homes were included among the health care workers who were
vaccinated in the first phase of the rollout.
Rosen et al. Israel Journal of Health Policy Research (2021) 10:6 Page 3 of 14

3. Israel’s experience in, and infrastructure for,
planning and implementing prompt responses to
large-scale national emergencies
4. The organizational, IT and logistic capacities of
Israel’s community-based healthcare providers (the
four health plans), which are all large and national
in scope
5. The availability of a cadre of well-trained, salaried,
community-based nurses who are employed directly
by the health plans
6. The tradition of effective cooperation between
government, health plans, hospitals, and emergency
care providers –particularly during national
emergencies –and the frameworks for facilitating
that cooperation
7. The existence of well-functioning frameworks for
making decisions about vaccinations and support
tools for assisting in the implementation of vaccin-
ation campaigns
8. The rapid mobilization of special government
funding for vaccine purchase and distribution
9. Timely contracting for a large amount of vaccines
relative to Israel’s population
10. The use of simple, clear and easily implementable
criteria for determining who had priority for
receiving vaccines in the early phases of the
distribution process
11. A creative technical response that addressed the
demanding cold storage requirements of the Pfizer-
BioNTech COVID-19 vaccine
12. Well-tailored outreach efforts to encourage the
population to sign up for vaccinations
These specific factors can be divided into three major
groups of factors, as follows:
A. Long-standing characteristics of Israel which are
extrinsic to health care (items 1–3)
B. Long-standing characteristics of the Israeli health
care system (items 4–7)
C. Specific actions taken as part of the COVID-19 vac-
cination effort (items 8–12)
We now provide additional information on each of
the specific factors listed above, providing context
and detail about the Israeli rollout not previously
published in a comprehensive fashion. We also briefly
cite examples of high-income countries in which
those factors were not present, as vetted by country-
specific experts who reviewed a draft of this article.
We do so to demonstrate that many of these factors
are neither trivial nor universal. We purposely do not
present a comprehensive analysis of what have been
the main influences on the speed of the rollout in
any other country. Such comprehensive analyses are
best carried out by experts writing about their own
countries.
A. Long-standing characteristics of Israel which are
extrinsic to health
1. Israel’s small size, in terms of both area and
population, its relatively young population, and its
relatively mild weather in December 2020
Israel has a population of 9.3 million. As a result,
the number of doses required
6
was a small fraction of
the overall global supply, giving Israel agility and
maneuverability in its purchasing. Meanwhile, Israel’s
small size (about the same as New Jersey)
7
and highly
urbanized population, minimized the transport and
storage challenges associated with the Pfizer-
BioNTech COVID-19 vaccine (henceforth referred to
as “the Pfizer vaccine”, for short). Inter alia, a single
state-of-the-art medical warehouse sufficed to store
the nation’s entire Pfizer vaccine reserve in the
requisite ultra-low-temperature freezers.
8
In addition,
high population density increased the number of
people who can easily access any particular
community-based vaccination site –an important ad-
vantage with regard to the Pfizer vaccine.
Moreover, Israel’s population is relatively young (ap-
proximately 12% aged 65 or over) [6], reducing the
amount of vaccine needed to rapidly vaccinate the bulk
of the 60+ population.
6
Israel’s vaccination program covers all persons covered by Israel’s
National Health Insurance Law as well as additional groups, such as
soldiers (who are entitled to health care via the IDF) and prisoners
(who are entitled to health care via the Prisons Law). Undocumented
migrant workers are not covered.The Palestinian Authority is
responsible for the health and health care of Palestinian residents of
Gaza and the West Bank. This includes responsibility for providing
vaccinations against COVID-19. Thus, in general, they are not in-
cluded as part of Israel’s vaccination program. In contrast, Palestinian
workers legally residing in Israel by virtue of a residence permit
granted to them as part of a family reunification procedure, as they are
covered by the NHI.
7
We recognize that several European countries have areas similar to
that of Israel. The intention here is to distinguish this characteristics of
Israel’s area primarily from those of the US, China, Canada and other
large-area countries.
8
To some extent, these freezers were on hand prior to the pandemic.
Others were purchased during 2020 in preparation for the expected
need to store large quantities of the Pfizer vaccine.
Rosen et al. Israel Journal of Health Policy Research (2021) 10:6 Page 4 of 14
And, with Israel being a small country geographic-
ally, the vast majority of aging and infirm Israelis ap-
parently have a younger adult family member living
in close geographic proximity,
9
who can accompany
them to a vaccination site, while providing moral sup-
port and transportation assistance. The relatively mild
December in Israel in 2020 also made it easier for
older people to get to vaccination sites.
These facilitating factors - Israel’s small size, a
mild winter, and a relatively youthful population -
did not exist in some high-income countries [8]. For
example, the US has a population of over 300 mil-
lion, greatly increasing the amount of vaccine needed
by that country. Canada faced the challenges of a
large geographic area and parts of the country in
which the population density is low [9]; these cre-
ated a need for more storage facilities, greater in-
vestment in transportation, and a need for many
more vaccination sites.
10
And several European
countries have populations in which 20% or more
are over age 65
11
[10], meaning that vaccination
coverage of the elderly would require a greater vac-
cine supply in terms of doses per population. Thus,
many countries faced opening conditions –in terms
of geography, population size, and age distribution -
that were substantially more challenging than those
faced by Israel.
2. Israel has a centralized national system of
government
12
(as opposed to a federal system of
government)
Israel does not have states or regions which have
independent decision-making authority on public
health issues. While it does have active, and largely
independent, local authorities and municipal govern-
ments, they play only a limited role in health care.
13
As such, coordination of a public health response
across different levels of government was not needed
and this may have allowed the Israeli government
more flexibility in designing its rollout. It also
provided clarity in that the national government had
the primary responsibility for the vaccination
campaign, in terms of planning, financing, and
implementation.
14
In contrast, several high-income countries have fed-
eral systems, with significant implications for how
public health efforts are organized. For example in
the US, public health is administered and regulated
primarily at the state level. On the other hand, it was
the federal government that was responsible for pro-
moting vaccine development, approving vaccines as
safe and effective, procuring vaccines from pharma-
ceutical companies, and distributing them among, and
to, states. This has led to some ambiguity regarding
who is responsible and accountable for the success of
the vaccination effort [11–14].
3. Israel has extensive experience in, and
infrastructure for, planning and implementing
prompt inter-sectoral responses to large-scale na-
tional emergencies.
Partly as a result of its challenging geo-political
position, Israel has for many years invested substan-
tially in preparing for large-scale emergencies,
whether they be related to security, natural disasters,
or health, based on an “all hazards”approach [15].
Inter-sectoral decision making bodies and implemen-
tation teams have been established, protocols have
been developed, staff have been trained, and drills
have been carried out. The scenarios for recent large-
scale drills (pre-COVID-19) have included those in
which large scale vaccination efforts had to be imple-
mented. In Israel, the large community based health
care providers –the health plans –are an integral
part of national emergency preparedness drills. In
addition, due to its security situation, Israel has
amassed substantial real-world experience in respond-
ing to large-scale emergencies.
In the post-911 world, Israel is not the only country
investing time, energy, and money in preparations for
large-scale emergencies. But it is probably the case that
few European and North American countries have as
much experience as Israel does in responding to real-
world emergencies and many of them apparently do not
maintain surge capacity (relative to their size), to the ex-
tent that Israel does. Widespread public understanding
that large-scale emergencies are not rare events may en-
hance the seriousness with which the public,
9
According to the 2009 Social Survey carried out by Israel Central
Bureau of Statistics, 79% of the elderly in Israel met at least once a
week with a family member who does not live with them in the same
household [7]. The comparable figure in the 2019 Social Survey was
77%.
10
Confirmed by Greg Marchildon, personal communication, January
2021.
11
These include 23% in Italy, 22% in Germany, and 20% in France
12
Sometimes referred to as a unitary system of government
13
Nonetheless, some of these local authorities made an important
contribution to the vaccination campaign by making large municipal
facilities available as vaccination sites.
14
Of course, even with a single level of government involved, there
were issues to be resolved about the distribution of responsibility
between various agencies of the national government, such as the
Ministry of Health, the IDF, the Knesset, the Prime Minister, and the
Cabinet. In the case of the vaccine campaign, these issues seem to
have been resolved effectively. This has not been the case regarding
other aspects of the pandemic response.
Rosen et al. Israel Journal of Health Policy Research (2021) 10:6 Page 5 of 14
Loading more pages...