1
ZuberA, etal. BMJ Open 2022;12:e045327. doi:10.1136/bmjopen-2020-045327
Open access
Does adherence to a quality indicator
regarding early weaning from invasive
ventilation improve economic outcome?
A single- centre retrospective study
Alexander Zuber,1,2 Oliver Kumpf,2 Claudia Spies ,2 Moritz Höft,2 Marc Deffland,2
Robert Ahlborn,3 Jochen Kruppa,1 Roland Jochem,4 Felix Balzer 1,2
To cite: ZuberA, KumpfO,
SpiesC, etal. Does adherence
to a quality indicator regarding
early weaning from invasive
ventilation improve economic
outcome? A single- centre
retrospective study. BMJ Open
2022;12:e045327. doi:10.1136/
bmjopen-2020-045327
►Prepublication history and
additional supplemental material
for this paper are available
online. To view these files,
please visit the journal online
(http://dx.doi.org/10.1136/
bmjopen-2020-045327).
Received 30 September 2020
Accepted 26 August 2021
1Institute of Medical Informatics,
Charité Universitätsmedizin
Berlin, Berlin, Germany
2Department of Anesthesiology
and Operative Intensive
Care Medicine, Charité
Universitätsmedizin Berlin,
Berlin, Germany
3IT Department, Charité
Universitätsmedizin Berlin,
Berlin, Germany
4Departments of Machine Tools
and Factory Management, TU
Berlin, Berlin, Germany
Correspondence to
Professor Felix Balzer;
felix. balzer@ charite. de
Original research
© Author(s) (or their
employer(s)) 2022. Re- use
permitted under CC BY- NC. No
commercial re- use. See rights
and permissions. Published by
BMJ.
ABSTRACT
Objectives To measure and assess the economic impact
of adherence to a single quality indicator (QI) regarding
weaning from invasive ventilation.
Design Retrospective observational single- centre study,
based on electronic medical and administrative records.
Setting Intensive care unit (ICU) of a German university
hospital, reference centre for acute respiratory distress
syndrome.
Participants Records of 3063 consecutive mechanically
ventilated patients admitted to the ICU between 2012 and
2017 were extracted, of whom 583 were eligible adults
for further analysis. Patients’ weaning protocols were
evaluated for daily adherence to quality standards until ICU
discharge. Patients with<65% compliance were assigned
to the low adherence group (LAG), patients with≥65% to
the high adherence group (HAG).
Primary and secondary outcome measures Economic
healthcare costs, clinical outcomes and patients’
characteristics.
Results The LAG consisted of 378 patients with a median
negative economic results of −€3969, HAG of 205
(−€1030), respectively (p<0.001). Median duration of
ventilation was 476 (248; 769) hours in the LAG and 389
(247; 608) hours in the HAG (p<0.001). Length of stay
(LOS) in the LAG on ICU was 21 (12; 35) days and 16 (11;
25) days in the HAG (p<0.001). LOS in the hospital was 36
(22; 61) days in the LAG, and within the HAG, respectively,
26 (18; 48) days (p=0.001).
Conclusions High adherence to this single QI is
associated with better clinical outcome and improved
economic returns. Therefore, the results support the
adherence to QI. However, the examined QI does not
influence economic outcome as the decisive factor.
INTRODUCTION
In the last decades, the need for quality
management (QM) in the hospital has been
growing. On one hand costs have been rising
and on the other patients, health insurance
and public pressure urge hospitals to improve
outcome and services by cutting or tying
reimbursement to valid quality indicators
(QIs).1 This is why in the medium and long
run quality- oriented reimbursement (pay
for quality) might change the hospital land-
scape.2 Economics of health have been estab-
lished widely in order to curb costs for the
national healthcare system. Many countries
introduced diagnosis- related groups (DRGs)
in order to pay on averaged costs and on a
generalised financial reimbursement per case
(fixed prices). Reimbursement for inpatients
is linked to DRG accounting and updated
annually based on reported data from
hospitals. The fee- for- service system induces
hospitals to improve internal processes as
reimbursement is predefined and to work
goal- oriented towards therapeutic aims.3
In modern medicine, a considerable part of
hospital costs arises from intensive care. The
cost structure of a tertiary German hospital
shows that ca. 20% of costs are generated
in intensive care units (ICUs).4 Especially,
mechanical ventilation is the main cost driver
in ICUs.5 Approximately 6% of the patients
in intensive care are affected by prolonged
Strengths and limitations of this study
►This is the first study evaluating whether a quality
indicator on weaning has effects on the economic
outcome parameters on a per case basis.
►Results of the cost unit accounting practice is well
established and is thus representative for a detailed
examination of unit costs.
►The test and validation sample was taken from a
reference centre specialised on acute respirato-
ry distress syndrome in adult patients with severe
medical conditions.
►Control for interactions with other quality indicators
is necessary as the examined quality indicator is po-
tentially connected with other ones.
►The study results are based on German reimburse-
ment system and might be typical for a tertiary
university hospital rather than German hospitals in
general

2ZuberA, etal. BMJ Open 2022;12:e045327. doi:10.1136/bmjopen-2020-045327
Open access
mechanical ventilation and weaning from mechanical
ventilation represents an essential element in the treat-
ment of critically ill patients as it can take up to 50% of the
ventilation time.6 As a consequence, up to 37% of all ICU
resources are allocated to these patients.7 This means that
weaning patients from mechanical ventilation is not only
essential for clinical outcomes like duration of ventilation
or length of stay (LOS),8 9 but also a critical step from an
economic perspective as costs can be reduced. Therefore,
this process is a critical phase in intensive care. However,
the ideal weaning process is still subject to debate.10
About 40% of patients receiving mechanical ventila-
tion will experience a complicated weaning process.11
Patients categorised in prolonged weaning, failing at least
three spontaneous breathing trials (SBTs) or receiving
more than 7 days of weaning after the first SBTs, have an
increased risk in developing hospital mortality, mainly
through ventilator- associated pneumonia (VAP),6 but also
through postintensive care syndrome (PICS) or chronic
critical illness (CCI).12 Due to demographic changes and
technological advances in intensive care, the number
of older patients with complex diseases or comorbidi-
ties needing ventilation is increasing.13 14 This generates
growing costs, as the cohort of patients requiring respira-
tory support accounts for a disproportionate percentage
of the resources available in intensive care.15
With the purpose of managing quality throughout the
difficult framework conditions of hospital care, a proactive
and structured QM is essential.16 In general, QM focuses
on securing and improving clinical services economi-
cally, performed by physicians or nurses according to the
patient’s needs.17 In Germany, in the context of European
and national QM initiatives, consensus- based standardised
QIs were developed for intensive care medicine since
2010—third version in 2017—by the German interdisci-
plinary society for intensive and emergency care (DIVI)
in order to simplify the measurement of relevant quality
data, to record timely and to allow transparent compari-
sons of patient data. The according quantification of QM
helps measuring effectiveness and efficiency of ICUs.18 19
QIs enable a descriptive picture of the actual condition
and are an indispensable instrument for comparisons
between different states of quality.18 Potentially, widely
accepted QIs can progress hospital economics and
support the reduction of the national budget for health-
care, even though a recent study has shown that cost–
quality relationships are difficult to generate.20
QIs empower advances in intensive care medicine to be
measured and evaluated on a regular basis.19 QIs can be
defined as representative figures for quality of structure,
processes or outcome within the medical care process.
Thus, indicators are useful for measuring improvement
in the context of QM and should be developed in line
with evidence- based literature.21 Ideally, measures for QIs
can be extracted from routine patient data to avoid excess
documentation work. Therefore, patient data manage-
ment systems (PDMS) are pivotal for measuring complex
quality figures.18 The economic aspects for the whole
hospital of the introduction of QIs are not well investi-
gated. However, the is evidence that the application of
QIs is a value- creating instrument.12
The objective of this study was, to determine the
economic impact of adherence to a single QI evalu-
ating the weaning process from invasive ventilation. We
analysed this by comparing economic results per case
and clinical outcome parameters like LOS between two
groups of either high- quality or low- quality adherence.
Additionally, we sought to determine factors that would
influence a potential interaction between economic and
outcome parameters.
METHODS
This original research is in accordance with the Consoli-
dated Health Economic Evaluation Research Standards.
Patient and public involvement
Patients and the public were not directly involved in this
observational study.
Study centre
We conducted this single study- centre in a university
hospital (Charité-Universitätsmedizin Berlin). This obser-
vational analysis was performed at a 14- bed ICU (refer-
ence centre), specialised in treatment of acute respiratory
distress syndrome in adult patients. All patients at our
ICU were treated according to guidelines and internal
standard operating procedures for clinical practice.22
Study design
This was a retrospective descriptive study, using data from
multiple electronic databases used in routine patient
care and for routine administrative purposes. All patients
admitted to and discharged from the ICU between
1 January 2012 and 31 December 2017 who received
invasive ventilation during their stay were eligible to be
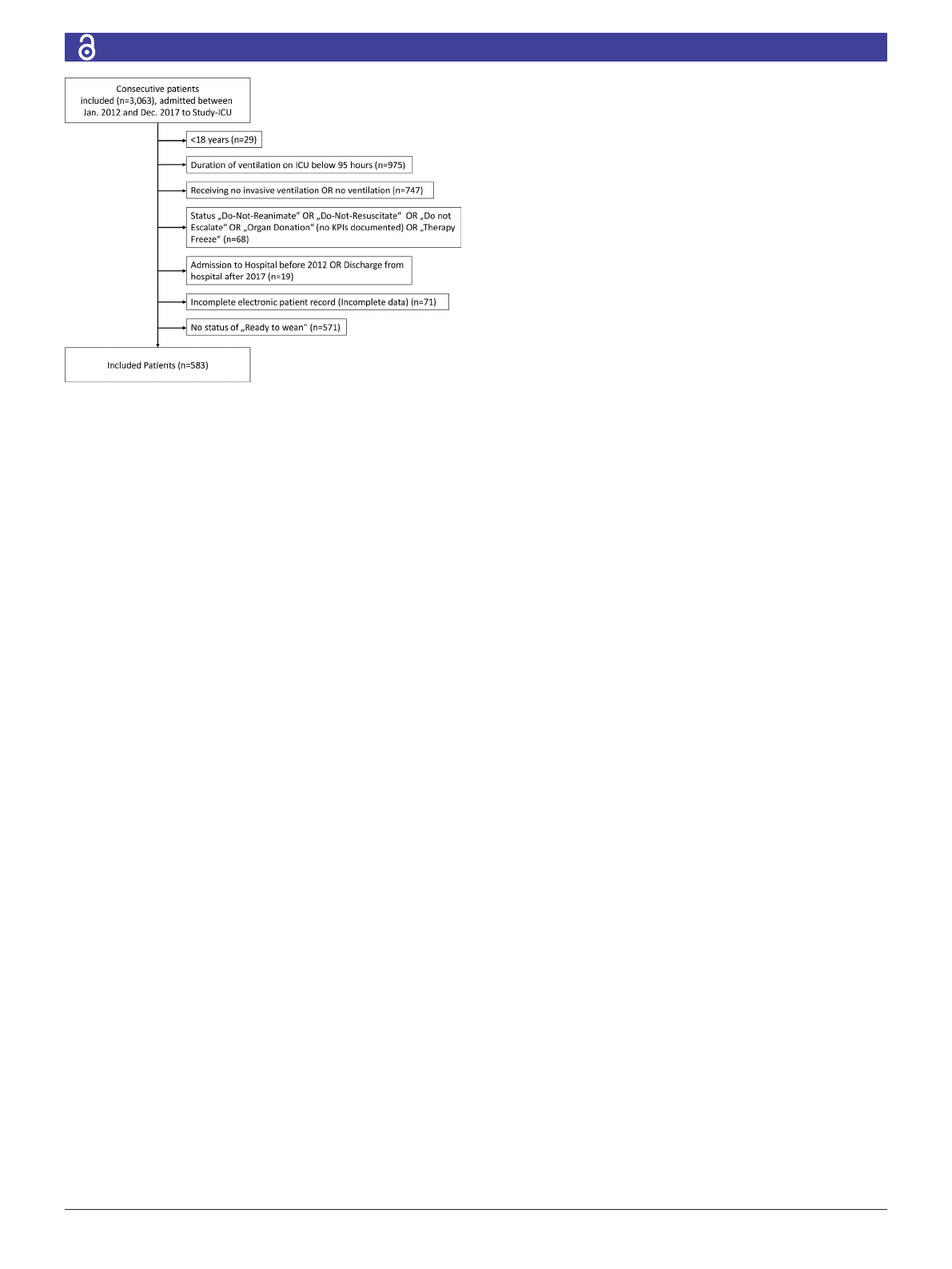
included in this study. Furthermore, duration of ventila-
tion <95 hours, receiving no invasive ventilation, terminal
status, incomplete patient record or missing readiness
to be weaned were defined as exclusion criteria (see
figure 1).
Confidentiality was guaranteed, no interventions were
performed and only clinical routine data were collected.
Data were retrieved from a PDMS called (Computer
Organised Patient Report Assistant; COPRA System,
Berlin, Germany). Data are recorded both automatically
by patient monitors and manually by caregivers. The ICU
staff validates all information manually. However, the
design of the PDMS prevents manual alterations to the
data, for example adding missing values after discharge
from the ICU. PDMS data are also transferred to the clin-
ical information and accounting system (SAP, Walldorf,
Germany). Based on this administrative system, cost unit
accounting is performed annually. In addition to basic
demographic data, we assessed clinical and administra-
tive parameters of in- patient cases (eg, LOS). Data were
3
ZuberA, etal. BMJ Open 2022;12:e045327. doi:10.1136/bmjopen-2020-045327
Open access
retrieved using a structured query. No patient identifiers
were extracted in order to secure anonymity of patients’
data. Data related to diagnoses were not retrieved from
the administrative systems.
PDMS data of patients included in the study were trans-
ferred to the study database, where we also collected the
administrative and cost accounting data, respectively. We
contrasted patient, intensive care and economic param-
eters of the two adherence groups (see table 1). Then,
we calculated the profits per case by subtracting costs
of reimbursement per case. In order to generate an
economic outcome per case for the dependent variable
in multivariate linear regression. Besides administrative
data, we used different scores for assessing the QI for eligi-
bility. Selection criteria were: (1) no additional workload
required for documentation, (2) the availability within
the PDMS system, (3) standardised values for all patients
and the existence of standard operating procedures for
each indicator and (4) the relevance of the indicator for
clinical decision making.19 23
Procedures
In this study, we used present key performance indica-
tors (KPIs) in order to examine the adherence to the
QI ‘Early Weaning from Invasive Ventilation’ until ICU
discharge.8 A small set of evidence- based KPIs was estab-
lished in 2009, providing indicators that were already
available within the PDMS. The KPIs in intensive care
medicine proved helpful for practical use and compliance
with standard operating procedures. A description of the
KPI is provided in online supplemental material. Within
the weaning therapy, fast visual feedback for ‘readiness
to wean’ and ‘weaning protocol compliance’ were imple-
mented. If both KPIs were positive, the according result of
the SBT was recorded.23 Once the patient was assessed to
be ready to wean since the primary disease showed clinical
improvement, the standard weaning protocol activities
were conducted on a daily basis according to standard
operating procedures. Congruent with clinical guidelines
in place, weaning protocols were adapted to evaluate the
progress of respirator therapy.22 The subsequent result
was recorded in the weaning protocol. For each patient,
we monitored the daily weaning protocol compliance
between readiness to wean and ICU- discharge in order
to evaluate the percentage of adherence. Within the
weaning process, the SBT represents the major diagnostic
test to evaluate if the patient can be extubated success-
fully.10 The SBT is successful if the patient succeeded
the trial and does not have to be re- intubated within 48
hours.24 This process is directly linked to a specific QI for
weaning derived from the DIVI- QI.19 A definition of the
indicator is presented in online supplemental material.
Outcome parameters
In this study, we investigated for economic results, clin-
ical outcome parameters per case and the respective
adherence to quality. Economic results were defined as
the profit or loss per case, by subtracting all assigned
costs from the reimbursement on a case level. Clinical
outcomes as a representative for clinical effectiveness
were measured in order to set economic outcomes in
relation to the purpose of medicine. Adherence to quality
was calculated on a per case level in order to categorise
the patients into groups.
We used the adherence level of the examined QI in
order to create two quality groups. We calculated the final
quality level by averaging the daily indicator results for the
duration with equal weights per day. In order to set the
optimal cut- off point for dichotomously distinguishing
between high- adherence and low- adherence of weaning
quality, we combined recommendations from literature
with our institutional standards. A cut- off value of 70%
deemed as a suitable fulfillment- threshold for QIs.25
However, due to partially high workload under certain
circumstances in intensive care, we decided to lower the
cut- off for 5% tolerance in order to account for missing
values in documentation. Therefore, we inserted a cut- off
for weaning protocol compliance at 65% adherence. The
low adherence group (LAG) was defined as adherence to
QI of less than 65%. The high adherence group (HAG)
was defined as adherence to QI of equal or more than
65%. Once this threshold was reached, the QI was charac-
terised as high adherence.
Statistical analyses
Descriptive analyses and statistical testing were
performed using SPSS, V.14.0 (SPSS) for Windows.
Results are expressed as median (IQR) or frequency
(%). We controlled data for risk and severity by exclusion
as patients and therapies in intensive care are hetero-
genic, as studies have shown.18 Differences between the
adherence groups in terms of outcome parameters were
tested using the univariate unpaired t- test and χ2 statistics
for independent variables as appropriate with a p<0.05
regarded as significant.
Figure 1 Patient inclusion and exclusion criteria. Flow chart
of the process used in this study for patient record inclusion.
Numbers listed are number of patients in each group. ICUs,
intensive care units; KPIs, key performance indicators.
4ZuberA, etal. BMJ Open 2022;12:e045327. doi:10.1136/bmjopen-2020-045327
Open access
In order to investigate the influencing factors in more
detail, parameters that were found to be statistically
significant on univariate analysis or out of discussion
among the experts underwent stepwise multivariate anal-
yses. We used multiple linear regression analyses to model
the relationship between the independent variables and
the outcome of profitability. Regression coefficients (95%
CI) and the corresponding p values were calculated for
each factor. Testing the dataset for outliers was performed
using the cook distance test, based on the model. The
test did not indicate the need to dismiss cases from the
sample. Due to an exploratory character of the research,
no adjustments for multiple testing were made.
RESULTS
All patients with complete electronic patient records
(n=3063 patients) were screened for eligibility. After
selection regarding inclusion and exclusion criteria, 583
patients were included in the final analysis (figure 1). Of
these patients, 378 showed low- adherence if the indicator
was below 65% and 205 showed high adherence. The
median age of admitted patients was 57 (40; 70) years;
64.7% of patients were male. There were significantly
(p=0.038) more male patients within the HAG (70.2%)
than in the LAG (61.6%). As reflected by a median Acute
Physiology and Chronic Health Evaluation II (APACHE
II) admission score of 21 (14; 27), a Simplified Acute
Physiology Score II (SAPS II) admission score of 47 (34;
61) and a Sequential Organ Failure Assessment (SOFA)
admission score of 9 (7; 12), the study population was
characterised by severe medical conditions. Patient
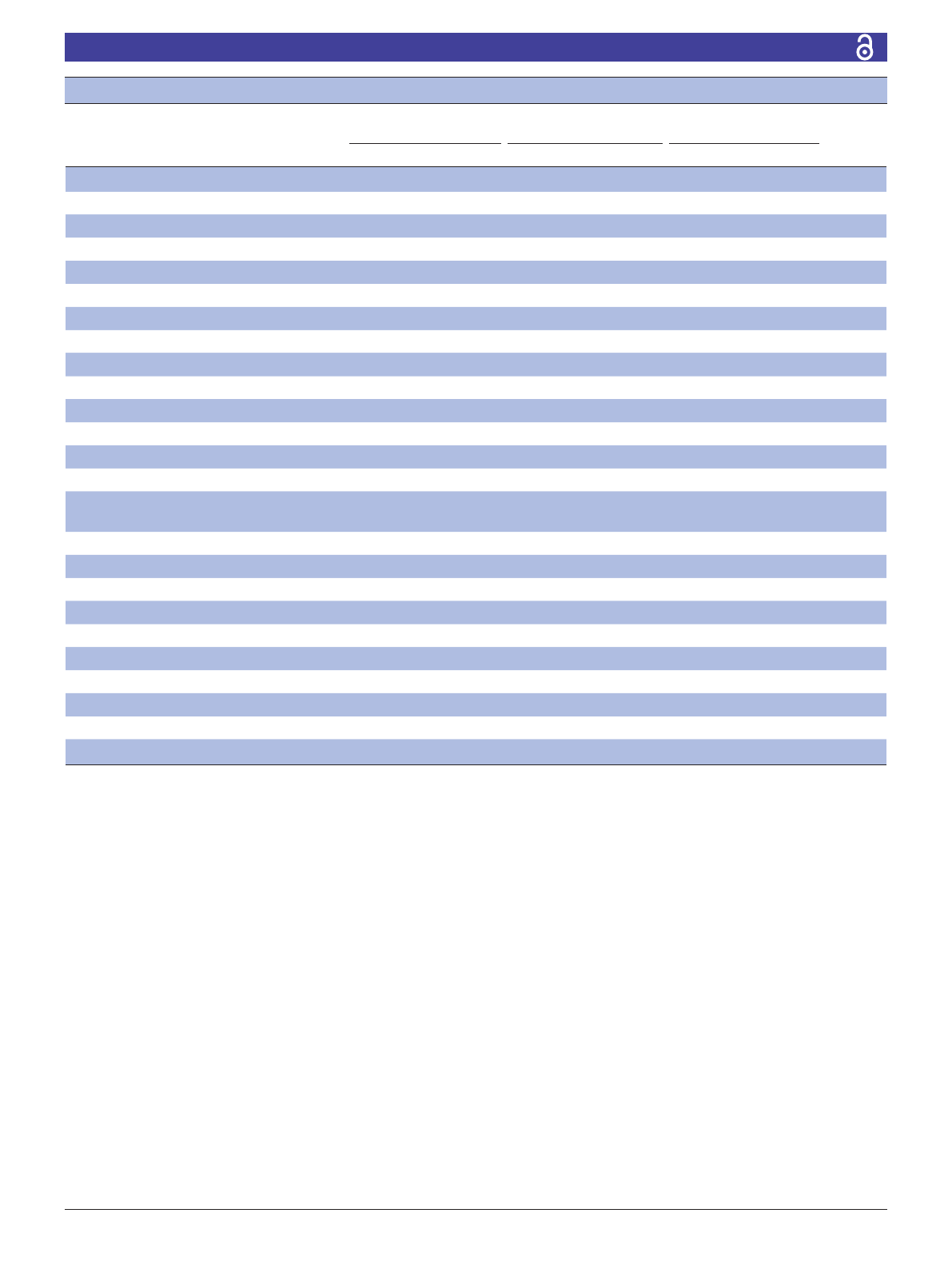
Table 1 Patient demographics and outcome parameters in comparison between QI adherence groups
All patients
LAG
QI <65%
HAG
QI ≥65%
P valuen=583 n=378 n=205
Demographics
Age (years) 57 (40; 70) 57 (40; 70) 55 (42; 69) 0.770
Gender (male) 377 (64.7%) 233 (61.6%) 144 (70.2%) 0.038
ICU score on admission
APACHE II 21 (14;27) 21 (15;27) 21 (14;27) 0.986
SAPS II 47 (34;61) 47 (35;60) 47 (34;62) 0.860
SOFA 9 (7;12) 9 (7;12) 9 (7;13) 0.526
Average SOFA 8.2 (6.6;10.3) 8 (6.5;10.1) 8.4 (6.8;10.7) 0.140
Type of admission to Study- ICU 0.651
Medical 290 (49.7%) 190 (50.3%) 100 (48.8%)
Emergency surgery 232 (39.8%) 146 (38.6%) 86 (41.9%)
Elective surgery 61 (10.5%) 42 (11.1%) 19 (9.3%)
Outcome parameter
Duration of Ventilation Study- ICU (hour) 431 (250;709) 476 (248;769) 389 (247;608) <0.001
Total duration of ventilation hospital
(hour)
578 (338;924) 597 (310;992) 535 (361;821) 0.017
No spontaneous breathing trials 1 (0;2) 1 (0;2) 1 (0;2) 0.456
No reintubation 0 (0;1) 0 (0;1) 0 (0;1) 0.531
Type of discharge of study- ICU <0.001
ICU 161 (27.6%) 100 (26.5%) 61 (29.8%)
Intermediate/ward 260 (44.6%) 172 (45.5%) 88 (42.9%)
Rehabilitation 110 (18.9%) 56 (14.8%) 54 (26.3%)
ICU mortality 52 (8.9%) 50 (13.2%) 2 (1.0%)
LOS Study- ICU (days) 19 (11;32) 21 12;35) 16 (11;25) <0.001
LOS hospital (days) 33 (20;54) 36 (22;61) 26 (18;48) 0.001
Profit (€)−2999 (−15 946; 7730) −3696 (−21 170; 6828) −1030 (−11 134; 9449) <0.001
Discrete variables are presented as a total number of encounters and were analysed with χ2 test for non- parametric samples.
APACHE II, Acute Physiology and Chronic Health Evaluation II; HAG, high adherence group; ICU, Intensive care unit; LAG, low adherence
group; LOS, Length of stay; QI, quality indicator; SAPS, Simplified Acute Physiology Score; SOFA, Sequential Organ Failure Assessment.

5
ZuberA, etal. BMJ Open 2022;12:e045327. doi:10.1136/bmjopen-2020-045327
Open access
demographics are displayed in table 1. Along the line, at
discharge patients generated an average daily SOFA score
of 8.2 (6.6.; 10.3) indicating resource- intensive moni-
toring and treatment of the patient.
In order to account for the remaining clinical patient
outcomes after grouping, we analysed the ventilation
parameters. Overall in the median, patients were venti-
lated for 431 (250; 709) hours on the ICU and 578 (338;
924) throughout their hospital stay. Following the divi-
sion into two adherence groups, there was a significant
reduction in duration of ventilation on ICU from 476 to
389 hours (p<0.001). Overall in- hospital duration of venti-
lation was decreased from 597 to 535 hours (p=0.017).
Concerning the number of SBTs and reintubations, there
was no significant finding (p=0.456 and p=0.531). In addi-
tion to the significant decrease in ventilation parameters
seen between the differences in adherence, the LOS was
decreased by 5 days from 21 to 16 (p<0.001) and overall
in- hospital LOS decreased from 36 to 26 days per patient
(p=0.001) in the median, indicating strong arguments
for QI adherence. With regard to economic outcome,
the overall median economic results (loss) per case was
−€2999. There was an increase in profitability from a
median loss of €3696–€1030 (p<0.001).
Considering the discharge of the patients, there was
a highly significant difference (p<0.001) between both
groups. Most patients were discharged to intermediate
care (44.6%), other ICUs (27.6%) or rehabilitation
(18.9%). Within the LAG, 50 (13.2%) patients died on
the ICU compared with 2 (1.0%) in the HAG. This gives
room to assume a certain impact of weaning quality on
mortality. However, since we did not include diagnosis
data, we cannot exclude an influence from this fact.
Multiple linear regression
The results of the multivariate linear regression analysis of
the complete study population of 583 patients are given
in table 2. The parameters were not adjusted for severity
of illness. The fixed variables age, sex and percentage of
QI adherence examined did not show significant effects
on profitability.
In the linear regression analysis, the LOS on the
study- ICU (p<0.001), the LOS in the hospital (p<0.001),
the averaged daily SOFA score (p<0.001) and the aver-
aged daily costs per patient (p<0.001) were shown to have
significant effects on the profitability (table 2). Strong
effects were found for the averaged daily SOFA score,
which increased profits per case by €1608 (95% CI €892
to €2323) for each SOFA point. Furthermore, the LOS
on the ICU decreased profits per case for €529 for every
day longer on the ICU. To the best of our knowledge,
multivariate regression for economic outcome has not yet
been conducted for these factors. The regression model
was performed without the admission scores for SAPS II,
SOFA and APACHE II. When these scores were included,
the statistical significances remained unchanged for the
remaining variables that were analysed (see table 2).
Comparing the cumulative parameters of weaning
patients along the years (see table 3), a higher number
of patients weaned as well as a higher average SOFA-
score can be associated with a higher number of median
economic result. The observation over time supports the
outcome parameters of table 1. Considering the develop-
ment since 2012, there is an increase in the number of
patients weaned per year and a decrease in the median
hours of ventilation per patient.
DISCUSSION
The most important finding was that clinical and
economic results were better within the HAG than the
LAG. We sought to evaluate whether adherence above
a certain quality threshold leads to a better economic
result per case for the hospital. Our univariate model
confirmed our hypothesis that higher quality leads to
better LOS and hospital costs of intensive care patients.
However, an improvement of the QI ‘early weaning’ was
not directly associated with a significant impact on the
profitability per case. In the regression model, we were
not able to prove that more quality lead to higher earn-
ings. Instead, significant factors were clinical outcome
parameters (LOS ICU, LOS Hospital and averaged daily
SOFA score), which had direct effects on profitability.
Moreover, these parameters were also superior within the
HAG, indicating a certain quality effect. This sequence of
effects shows that quality affects the economic results indi-
rectly via clinical outcome. This means that quality leads
to clinical efficiency. Literature already proposes a more
effective use of the costly resource ICU.26 Thus, from
an economic perspective it is recommended to transfer
patients as early as possible from ICU downstream (eg,
intermediate care) since a prolonged ICU- stay might be
inappropriate, dangerous and costly.23 25
Highly specialised ICUs are resource- intensive and cost-
intensive and not universally available. By implementing
QM as a method to constantly eliminating the factors
Table 2 Multiple linear regression analysis of factors
affecting the profit of 583 intensive care patients who
underwent the weaning process
Variable B (95% CI) SE P value
Age (years) −16 (−119 to 87) 52 0.765
Gender (male) 1139 (−2628 to 4906) 1918 0.553
Quality (%)* 3732 (−2457 to 9920) 3151 0.237
LOS Study- ICU (days) −529 (−671 to −387) 72 <0.001
LOS hospital (days) −143 (−213 to −71) 36 <0.001
Reintubations −928 (−2.457 to 602) 779 0.234
Average SOFA 1608 (892 to 2323) 364 <0.001
Daily costs (€)−7.6 (−11 to −4) 2 <0.001
*Quality, adherence to the quality indicator ‘early weaning from
invasive ventilation’.
ICU, intensive care unit; LOS, length of stay; SOFA, Sequential
Organ Failure Assessment.
Loading more pages...