
1
29
4 Teleconsultation to
Improve Epilepsy
Diagnosis and Therapy
Krüger, Björn 1
Weber, Christian 2
Müllers, Johannes 1
Greß, Hannah 1
Beyer, Franziska 2
Knaub, Jessica 2
Pukropski, Jan 1
Hütwohl, Daniela 3
Hahn, Kai 4
Grond, Martin 3
Jonas, Stephan 5
Surges, Rainer 1
1 University Hospital Bonn, Department of Epileptology
2 University of Siegen, Institute of Knowledge Based Systems and
Knowledge Management
3 Klinikum Siegen, Department of Neurology
4 University of Siegen, Department of Electrical Engineering and
Computer Science
5 University Hospital Bonn, Institute of Digital Medicine
ORCID:
Krüger, Björn: 0000-0002-1596-6487
Weber, Christian: 0000-0001-6606-5577
Müllers, Johannes: 0009-0000-4883-4459
Greß, Hannah: 0009-0009-7841-5111
Knaub, Jessica: 0009-0000-4308-3094
Pukropski, Jan: 0000-0002-8280-6475
Jonas, Stephan: 0000-0002-3687-6165
Surges, Rainer: 0000-0002-3177-8582
30
4Introduction
The successful diagnosis of epilepsy necessitates close collaboration
between physicians like general practitioners, pediatricians, neurolo-
gists and epileptologists. Pfäfflin et al. (2020) summarized in a review
study based on direct surveys of healthcare professionals that the
estimated prevalence of treated epilepsy in Germany was 4.7 per 1000
individuals in 1995 and increased to 5.5 per 1000 individuals in 2010.
“The estimated number of patients referred to or treated by neurolo-
gists increased from 193,000 to 266,000.” (Pfäfflin et al., 2020). In 2022,
the German Brain Foundation approximated that “10 percent of all
individuals experience a seizure in their lifetime, with approximately
0.6 percent affected by epilepsy.” (Deutsche Hirnstiftung, 2022)
Of utmost importance is the continuous exchange and
enrichment of available specialized knowledge. The German Society
of Epileptology emphasizes from a reverse perspective, “a substantial
part of the epilepsy problem lies in the fact that existing knowledge
about epilepsy is not being applied.” (Deutsche Gesellschaft für Epi-
leptologie e.V.) Teleconsultations have the potential to significantly
enhance the application of existing knowledge in epilepsy beyond
specialized centers. By facilitating remote communication between
healthcare professionals, teleconsultations break down geographical
barriers, ensuring that individuals in remote or underserved areas
have access to the latest advancements in epilepsy care. Feldmeier et
al. (2022) showed that teleconsultations were well received by patients
and that they “appreciated the time saved and the organizational con-
venience compared to a visit to a university outpatient clinic”. In the
following exploration, we will delve into the potential improvements
that teleconsultations can bring to various processes, examine the
necessary requirements for their successful implementation, and high-
light emerging research questions stemming from the introduction of
teleconsultation services.
Promoting Exchange with Teleconsultation
The continuous exchange of specialized knowledge and treatment
experiences, and the resulting essential connection of expertise, are
vital for the anamnesis, diagnosis, and ongoing support necessary for
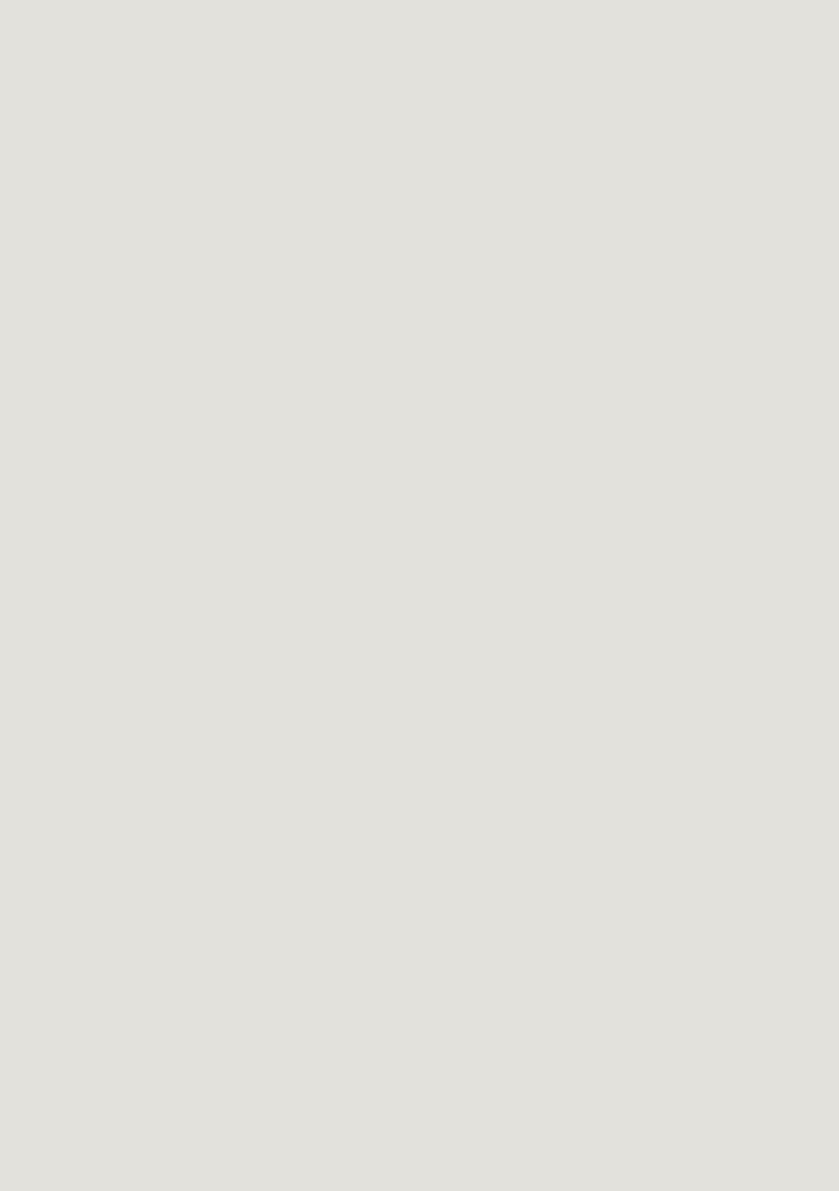
early recognition and long-term reduction of personal suffering. Fig-
ure 1 outlines a typical process without possibility of teleconsultation.
Patients with suspicion of epilepsy can be referred to non-specialized
clinics (local clinic) by general practitioners or emergency services and
31
4undergo locally established anamnesis interviews. They are diagnosed
by local physicians, naturally with a bias on the clinic’s specialization.
Patients may receive initial medication treatment, and are referred
back to the general practitioner, or in severe cases to a specialized
center for seizure disorders (specialized clinic). Appointments for ex-
aminations and referrals may be associated with varying and extended
waiting times that are not well-aligned with the individual urgency.
This diagnostic delay is to the patient’s disadvantage, as it can lead to
anxiety, confusion, and frustration on a personal level, and in more
severe cases to misdiagnosis and progression of untreated seizure
condition (Alessi et al., 2021). Consultation with specialists are neces-
sary for a confirmed diagnosis, since cases in the context of epilepsy
are highly unique.
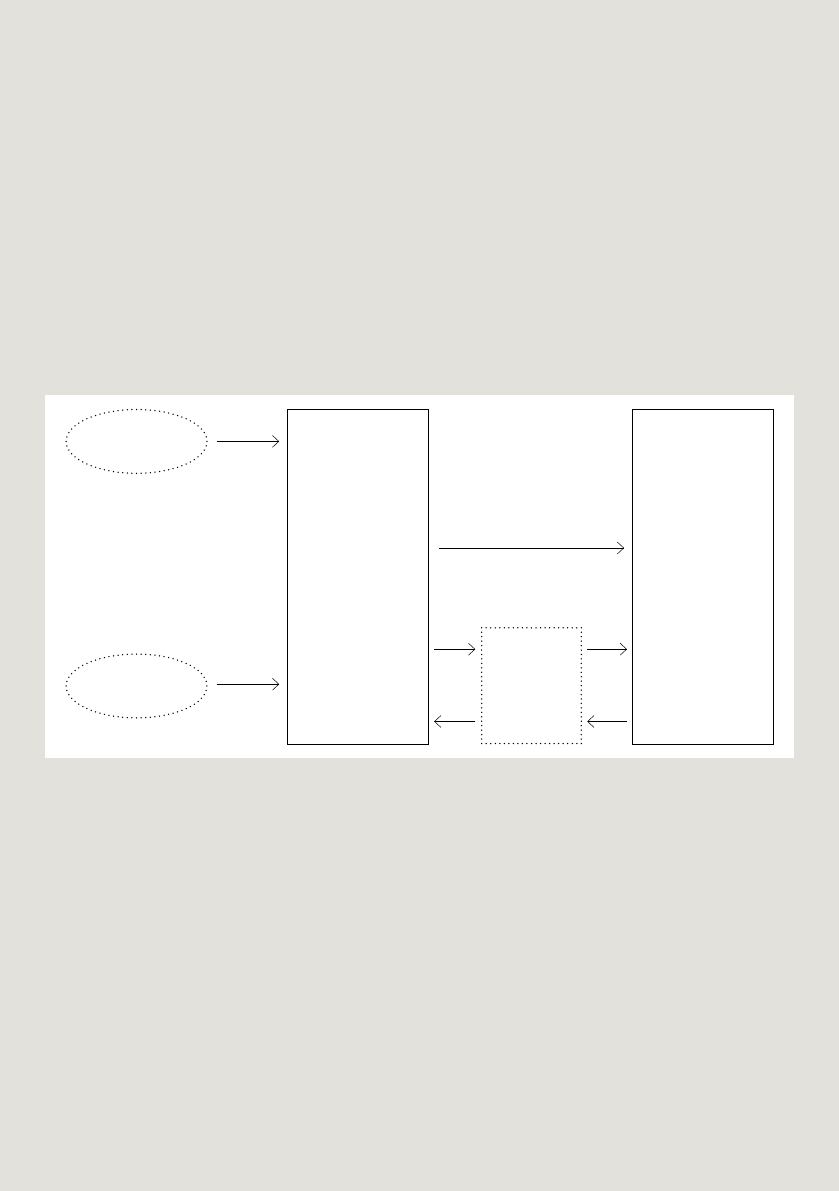
Employing teleconsultation between a local clinic and a specialized
clinic is outlined in Figure 2. The local clinic can rely on diagnostic
assistance from the specialized clinic and start an appropriate therapy,
possibly with no need to transfer the patient to the specialized clinic.
This will benefit the patient, the local clinic, and the specialized clinic.
The patient will undergo medically sensible examinations and receive
tailored therapy. The local clinic can focus their resources based on
effective recommendations from the specialized clinic and assimi-
late knowledge in the process. The specialized clinic might be able to
provide care for a patient who might otherwise have to be transported
and admitted to it.
local
clinic
admission
anamnesis
diagnosis
therapy
general
practicioner
emergency
services
specialized
clinic
admission
anamnesis
diagnosis
therapy
general
practicioner
further
treatment
referral
after seizure
dis-
charge
Figure 1: Process without teleconsultation.
transfer
referral
follow-
up visit
dis-
charge
32
4
Focusing on clinical processes, we specifically see the following po-
tential benefits arising from a teleconsultation: 1. Ruling out differen-
tial diagnosis such as syncopes or dissociative disorders. 2. Identifying
treatable causes for epilepsy (e.g. autoimmune inflammation).
3. Collective assessment of therapy options during the different stages
of the condition (onset, after second medical trial, in chronic phase).
4. Collective evaluation of additional diagnostic tests (such as electro-
encephalography (EEG) and magnetic resonance imaging (MRI), which
require specific expertise for interpretation. 5. Enhanced preparation
for referrals through additional examinations that can be conducted
locally during waiting times at the local clinic.
Requirements for Teleconsultation
Teleconsultation is often technologically limited, meaning only a
procedure for e-mails, phone, or video calls is established, and the
document exchange is limited to specific file formats or a specific
platform, making it impossible or tedious to share and evaluate patient
data. We want to outline the requirements for a modern teleconsul-
tation. The technological basis for any teleconsultation is a secure
channel between both parties, usually realized by a virtual private
network (VPN). This secure channel may be provided by an exter-
nal company responsible for the software solution, or the clinic’s IT
department, or another entity. The exchange of data between clinics
is not straight-forward, as there is no nationwide all-in-one solution
Figure 2: Process with teleconsultation.
local
clinic
admission
anamnesis
therapy
general
practicioner
emergency
services
specialized
clinic
diagnosis
recommendation
for therapy
general
practicioner
further treatment
tele-
consultation
request
tele-
consultation
response
referral
after seizure
discharge
33
4offering to transfer all required data through one platform. The project
“Virtuelles Krankenhaus Nordrhein-Westfalen”, which uses the elec-
tronic case file (Elektronische Fallakte, EFA) to share data (Dohmen et
al., 2021), might be a promising solution in the future. At this time, the
project is limited to only a few specialized departments and is current-
ly not available for epilepsy specialists, but represents an expandable
base structure for epilepsy support.
Medical patient data, such as master data, anamnesis
and recorded vital parameters, are saved in the hospital’s hospital
management system (Krankenhausinformationssytem, KIS). Direct
sharing between two KIS is feasible if hospitals use the same product,
or exchange through a common standard (Health Level Seven (HL7),
Fast Health Interoperability Resources (FHIR)). Expert exchanges have
shown that in many teleconsultation projects, data still has to be cop-
ied manually into a separate forms, hindering the acceptance by medi-
cal personnel and increasing the risk of errors in the manual process.
Anamnesis needs to be standardized to guarantee a
streamlined communication between the involved partners. Such stan-
dards ensure that already in first consultations, relevant base informa-
tion for a distributed diagnosis are collected to minimize communica-
tion overhead between the requesting and specialized clinic, as well as
preventing repeated anamnesis. In addition, the process of standardiz-
ing the anamnesis already transfers first knowledge to the requesting
entity by raising awareness for critical questions and observations.
Image data, such as computed tomography (CT) and
MRI, are saved in a picture archiving and communication system
(PACS) in the Digital Imaging and Communications in Medicine (DI-
COM) format, with the same implications as for KIS: Sharing between
the hospitals may be possible with little or no obstacles, or it is again
required to export data and send it through another platform. In the
case of epilepsy, EEG traces and associated surveillance videos are of
high interest. They often use proprietary formats with no standardized
way to exchange them between hospitals that are equipped by differ-
ent vendors. It is either necessary for both sides of the teleconsulta-
tion to have respective viewers or software licenses, or the data needs
to be converted into the DICOM format (Lang et al., 2023; Halford et
al., 2021).
Even in cases where processes are established on the
technological side, taking into consideration all points mentioned
above, teleconsultation can be hindered by missing training or limited
acceptance by medical personnel. Thus, it is indispensable to include
medical staff into the planning stage of any teleconsultation project.
Especially user interfaces and user experience have to be catered to
Loading more pages...