
sensors
Article
Reactive Exercises with Interactive Objects: Interim Analysis of
a Randomized Trial on Task-Driven NMES Grasp
Rehabilitation for Subacute and Early Chronic Stroke Patients
Andrea Crema 1,* , Ivan Furfaro 1, Flavio Raschellà 1, Mauro Rossini 2, Johannes Zajc 3,
Constantin Wiesener 4, Walter Baccinelli 5, Davide Proserpio 2, Andreas Augsten 6, Nancy Immick 6,
Sebastian Becker 7, Matthias Weber 7, Thomas Schauer 4, Karsten Krakow 6, Giulio Gasperini 2,
Franco Molteni 2, Michael Friedrich Russold 3, Maria Bulgheroni 5and Silvestro Micera 1,8,*
Citation: Crema, A.; Furfaro, I.;
Raschellà, F.; Rossini, M.; Zajc, J.;
Wiesener, C.; Baccinelli, W.;
Proserpio, D.; Augusten, A.;
Immick, N.; Becker, S.; Weber, M.;
Schauer, T.; Krakow, K.; Gasperini, G.;
Molteni, F.; Russold, M.F.;
Bulgheroni, M.; Micera, S. Reactive
Exercises with Interactive Objects:
Interim Analysis of a Randomized
Trial on Task-Driven NMES Grasp
Rehabilitation for Subacute and Early
Chronic Stroke Patients. Sensors 2021,
21, 6739. https://doi.org/10.3390/
s21206739
Academic Editors: Kei Masani,
Milos Popovic and Samuel C. K. Lee
Received: 23 August 2021
Accepted: 5 October 2021
Published: 11 October 2021
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
Copyright: © 2021 by the authors.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
1Translational Neural Engineering Laboratory, Center for Neuroprosthetics, Campus Biotech, EPFL,
2Centro di Riabilitazione “Villa Beretta”, Unità Complessa di Medicina Riabilitativa Ospedale Valduce,
3Ottobock HealthCare Products GmbH, 1110 Vienna, Austria; [email protected] (J.Z.);
[email protected] (M.F.R.)
4Technische Universität Berlin, Fachgebiet Regelungssysteme, 10587 Berlin, Germany;
5ABACUS s.r.l., 20155 Milan, Italy; [email protected] (W.B.); [email protected] (M.B.)
6Asklepios Neurological Clinic Falkenstein, 61462 Königstein-Falkenstein, Germany;
7HASOMED GmbH, 39114 Magdeburg, Germany; [email protected] (S.B.);
[email protected] (M.W.)
8The BioRobotics Institute and Department of Excellence in Robotics and AI, Scuola Superiore Sant’Anna,
56025 Pontedera, Italy
*Correspondence: andrea.cr[email protected] (A.C.); [email protected] (S.M.)
Abstract:
Enriched environments and tools are believed to promote grasp rehabilitation after stroke.
We designed S2, an interactive grasp rehabilitation system consisting of smart objects, custom
orthoses for selective grasp constraining, and an electrode array system for forearm NMES. Motor
improvements and perceived usability of a new enriched upper limb training system for sub-acute
stroke patients was assessed in this interim analysis. Inclusion criteria: sub-acute stroke patients
with
MMSE >
20, ipsilesional
MI >
80%, and contralesional
MI <
80%. Effects of 30-min therapy
supplements, conventional vs. S2 prototype, are compared through a parallel two-arms dose-matched
open-label trial, lasting 27 sessions. Clinical centres: Asklepios Neurologische Klinik Falkenstein,
Königstein im Taunus, Germany, and Clinica Villa Beretta, Costa Masnaga, Italy. Assessment scales:
ARAT, System Usability, and Technology Acceptance. Methodology: 26 participants were block
randomized, allocated to the study (control
N=
12, experimental
N=
14) and underwent the
training protocol. Among them, 11 participants with ARAT score at inclusion below 35, n = 6
in the experimental group, and n = 5 in the control group were analysed. Results: participants
in the enriched treatment group displayed a larger improvement in the ARAT scale (+14.9 pts,
pval =
0.0494). Perceived usability differed between clinics. No adverse effect was observed in
relation to the treatments. Trial status: closed. Conclusions: The S2 system, developed according to
shared clinical directives, was tested in a clinical proof of concept. Variations of ARAT scores confirm
the feasibility of clinical investigation for hand rehabilitation after stroke.
Keywords: sub-acute; stroke; interactive; grasp; rehabilitation
Sensors 2021,21, 6739. https://doi.org/10.3390/s21206739 https://www.mdpi.com/journal/sensors

Sensors 2021,21, 6739 2 of 17
1. Introduction
Stroke is the leading cause of disability in developed countries. Impairment affects
the large majority of stroke survivors and most of them require rehabilitation. Effective
treatment is timely required to avoid the learned non-use of the affected arm [
1
,
2
]. In-
creased life span in developed countries, and lowered averaged age of first stroke translate
into higher occurrence of stroke, longer disability-adjusted life expectancy, and higher
cumulative post-stroke assistance [
3
,
4
]. More recently the COVID-19 pandemic caused a
surge in the stroke population [
5
–
7
] and is expected to substantially modify the scenarios
of treatment and social care [
8
]. If not treated properly, stroke survivors need constant
external assistance even in basic daily activities. Environmental and personal factors can
hugely affect patients’ reactions and expectations [9,10] in the acute and sub-acute phase.
Upper-limb paresis is the most common of a sequelae of impairments following a
stroke, yet an effective treatment able to counter sensation of pain, feeling of foreignness,
muscle weakness, and spasticity is still an open issue. NeuroMuscular Electrical Stimu-
lation (NMES) is one of the treatments used to revert the learned non-use of the affected
limb, and to improve grasp capabilities [
3
] in severe hemiplegic patients. However, current
NMES systems have shown important limitations during unsupervised clinical use [
11
].
In a previous work [
12
] we designed a custom wearable device able to induce different
types of hand grasps by selectively stimulating extrinsic and intrinsic hand muscles. This
was possible due to the exploitation of spatial resolution features of the electrode array on
extrinsic and intrinsic hand muscles.
We designed an improved version of our device to comply with updated clini-
cal and technological requirements, and to support unsupervised task-driven clinical
tests. A preliminary test with a cohort of sub-acute stroke survivors was performed in
two clinical centres.
Historically, NMES systems have been tested primarily with chronic patients whereas
studies on patients in the acute and sub-acute phases are more limited [
13
,
14
]. The proximal
to distal gradient of motor and sensory deficits, and its longitudinal evolution after the
event, do also affect the statistical availability of treatable patients in the conventional
time windows for sub-acute and chronic stroke. For these reasons, the correct allocation
of treatment of the distal segments is not necessarily obvious within the personalized
clinical picture of the patient. However, post-stroke brain’s enhanced sensitivity to external
treatments suggests that the anticipation of a treatment may result in better improvement
for the patients. In particular, it is hypothesized that early treatment may provide improved
motor rehabilitation over conventional chronic treatment because it avoids the learned
non-use phase, and because treatment is provided in a recovery phase dominated by
high cortical plasticity. However, enriched grasp exercises designed for chronic patients’
treatments are usually not suitable for the sub-acute phase.
In the next sections we describe the design process, the technological outcome, and
clinical outcome of the interim analysis. Specifically, in Materials and Methods, we first
describe the methodology for the iterative design and validation with clinicians, caregivers,
and patients. The interaction of the central controller with orthoses, electrodes, stimulator,
and environmental sensing elements is described, alongside with the modality of operations
of each subcomponent. The description of a training session is then introduced. Finally,
we analyse the interim data both in terms of patients’ outcome, and through a usability
analysis of the whole assembly. One of the clinics involved in previous trials [
12
,
15
] is
taken as a benchmark for expert clinics with solid technical and technological know-how; a
second clinic, not previously exposed to similar technologies is used as a benchmark for
clinics with limited confidence with these prototypes. In the results, we show global and
treatment-specific motor improvements in patients. Moreover, we extrapolate indicators
suggesting that the challenge posed by an exercise is a determinant factor in the perceived
usefulness of the described device.
Sensors 2021,21, 6739 3 of 17
2. Materials and Methods
2.1. Methodology for the Design of the System Concept
The neuroprosthetic system was designed to rehabilitate hand functions through
passive and active components. Passive wearables allow selective wrist and finger motion,
and Electrode Arrays (EAs) induce controlled hand opening and closing via NMES. User-
centred methodologies were used throughout the design phase; usability requirements
were updated and refined during each development and verification phase. Physicians and
neurologists, directly involved in the project, provided high-level clinical specifications; the
bioengineering unit of one clinic further refined technical specifications. Two clinical focus
groups—one with physicians not directly involved in the project, and one with patients and
caregivers—were provided with an overview of the proposed system via a presentation
and demonstration of looks-like prototypes of the sensorized orthoses. Questions raised
during the demonstration were further addressed by the research technical staff and the
hospital technical staff provided the updated requirement lists. In further steps, therapists
suggested further changes. The resulting sub-components—Wearable NMES Orthosis,
Graphical User Interface (GUI) for Virtual Electrodes (VE), Control Interface (CI), smart
objects for environmental interactivity, Embedded Control System (ECS), and stimulation
apparatus—are detailed in the following sections.
2.2. Technological Implementation
The wearable NMES system uses topographically mapped multiple EAs, and acts as
a modular tool usable for grasp rehabilitation. Three independent EAs are positioned on
the forearm target extrinsic grasp muscles. An external stimulator with demultiplexers
delivers stimulation patterns that can be manually tuned to elicit functional grasp, to
obtain whole muscle conditioning, and to produce open-loop or closed-loop grasp control.
Custom orthoses selectively constrain fingers and wrist, grasp force and hand kinematics
are estimated through force and inertial sensors. The system interacts with daily-life objects
able to supply information (e.g., the object’s physical characteristics, expected sequence of
use) to drive their usage. The objects are equipped with radiofrequency sensitive passive
tags, and a reader embedded in the system processes the associated information in order to
run predefined sequences of actions. A devoted processing of the signal strength received
from the tags and environmental constraints allows the recognition of the selected objects
among others. The device control software is implemented in two main elements: (i) a
master CI operates on a windows tablet, and (ii) a real-time compliant ECS implementing
a deterministic state machine aimed at the control of the stimulation apparatus and of the
wearable NMES hand orthosis. This concept is exploited to drive rehabilitation exercises to
obtain deeper knowledge on the recovery of the patient. Figure 1depicts an overview of
the architecture.
2.2.1. Wearable for NMES and Object Interactivity
We updated a previous prototype [
12
] by included symmetric, reconfigurable compo-
nents that can be dynamically mapped, and driven by a novel stimulator. The new system,
visible in Figure 2, includes EAs that target hand extrinsic muscles, with active sites and
reference electrodes symmetrically positioned for usability with left and right arm. The
minimal electrode size was chosen to selectively target patients with small anthropometry.
Independent electrodes acting as active sites are sized 10
×
12
mm2
, and grouped in 4 by
4 arrays. Electrodes sized 20
×
40
mm2
—acting as reference—are positioned on opposite
sides. EAs can be composed to create larger structures of custom shape. Medical-grade
silver is screen-printed on functionalised polyester substrates. Electrodes are shaped in
four-by-one independent rows to improve local flexibility. High-tack gel, die cut to shape,
provides mechanical and electrical contact between skin and electrode.
Sensors 2021,21, 6739 4 of 17
2.2.2. Orthoses and Sensorized Components
Post-stroke flaccidity, appearance of spasticity, and onsets of pathological synergies [
16
]
affect the execution of complex movement combinations. In sub-acute patients, variations
across these stages can be frequent, and need to be accounted for on a per session basis.
We designed modular constraining orthoses to accommodate the expected lack of hand
control while preserving the grasp capabilities of the subjects, and the tactile afferences that
patients rely on during grasp. The Type-A orthosis, visible in Figure 2panel C, is aimed
at constraining wrist and fingers control. Five sizes account for forearms ranging from
200 mm to 350 mm. The dorsal side of the forearm is covered for two thirds of its length, as
well as the hand dorsum. In standard conditions the orthosis locks the wrist in extended
positions at 15
°
, and sets the thumb in slight opposition to the other fingers. However, all
rigid parts can be be heated with hot water and reshaped as needed. Rigid parts are foam
padded (OttoBock, Plastazote) for improved comfort. Finger clasps and rings, made of
thermoplastic rubbers, bind the fingers together and lock the thumb to the orthosis. Clasps
and rings host Inertial Measurement Units (IMU) (TDK InvenSense, MPU9250), and force
sensors (Tekscan Flexiforce, A201-A401). The Type-B orthosis, Figure 2panel D, is only
aimed at monitoring hand-wrist kinematics.
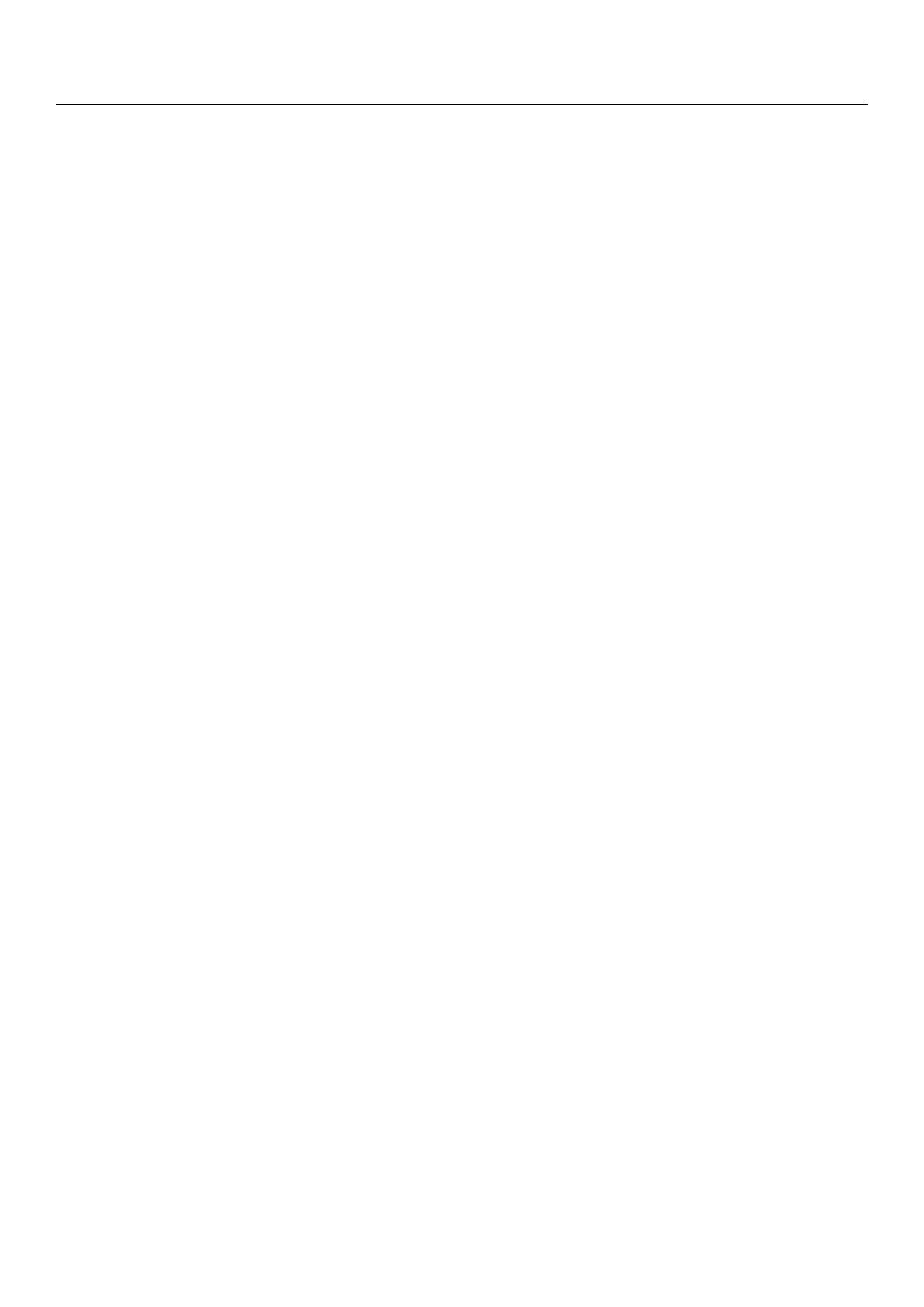
Figure 1.
Architecture of the system. The prototype operates in three different domains (i) envi-
ronmental interactivity (white), (ii) non-real-time control (teal), and (iii) real-time control (yellow).
Devices in the real-time domain operate synchronously at fixed frequency with no jitter. Non real-
time components operate at different frequencies aimed at giving a sensation of responsiveness but
absence of jitter is not guaranteed. The controller interface (CI) operates as an exercise controller,
logger, GUI for operators, and information broker from objects (Bluetooth) and RealTimeData. A
multilayer master–slave architecture combines non-real-time components (CI) with real-time compo-
nents managed by the Embedded Control System (ECS). ECS and CI share data and commands with
a custom instruction set over UDP. The ECS controls the set of IMUs via I2C, and the stimulation
apparatus via Virtual COM Port, and an on-board ADC for sampling grasp forces. Environmental
interactivity is dependent on synchronous real-time information and control fed at 40 Hz (hand
kinematics, thumb contact force, and pulse by pulse stimulation), and non real-time information
(3–5 Hz) from RF passive tags.
Sensors 2021,21, 6739 5 of 17
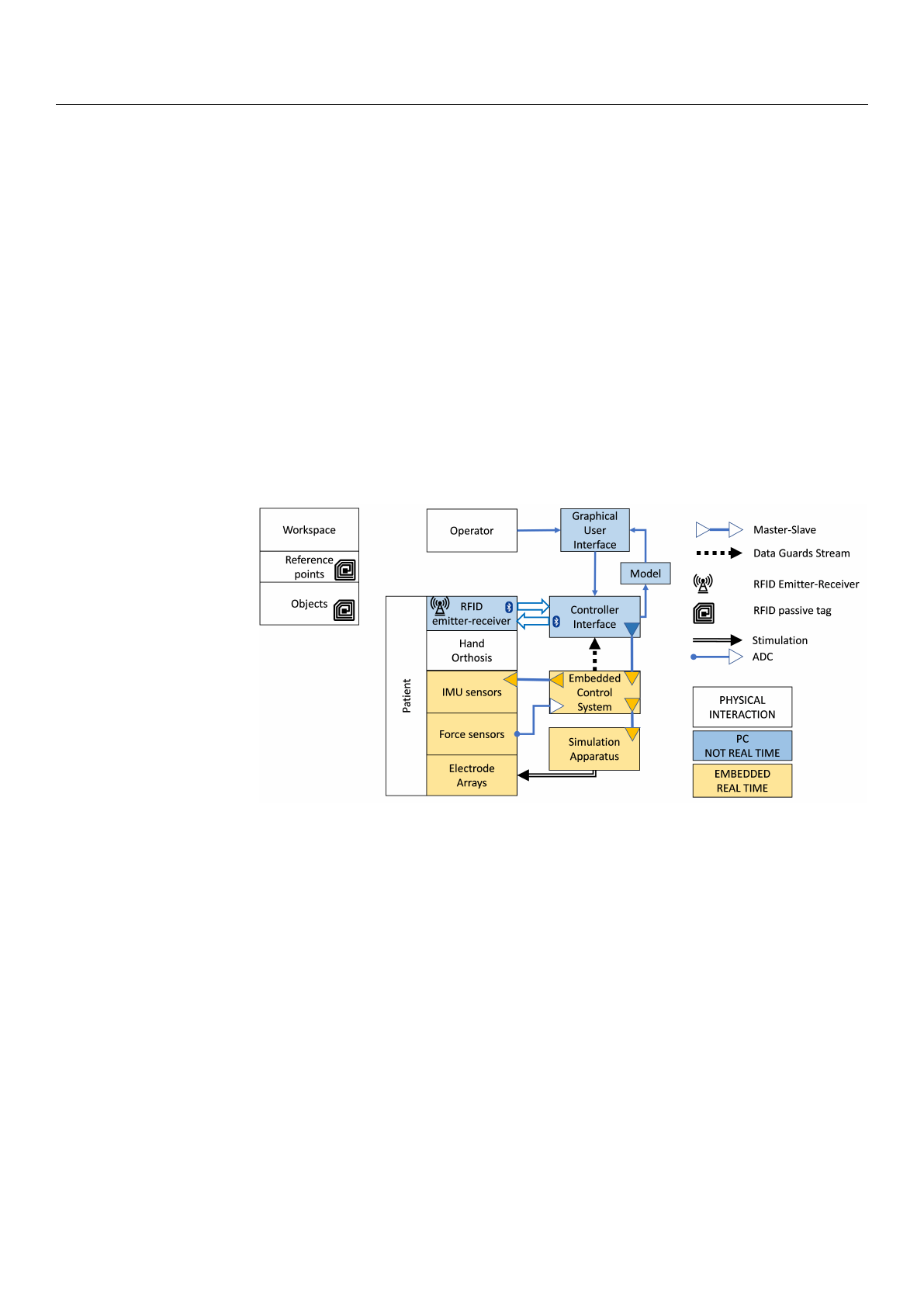
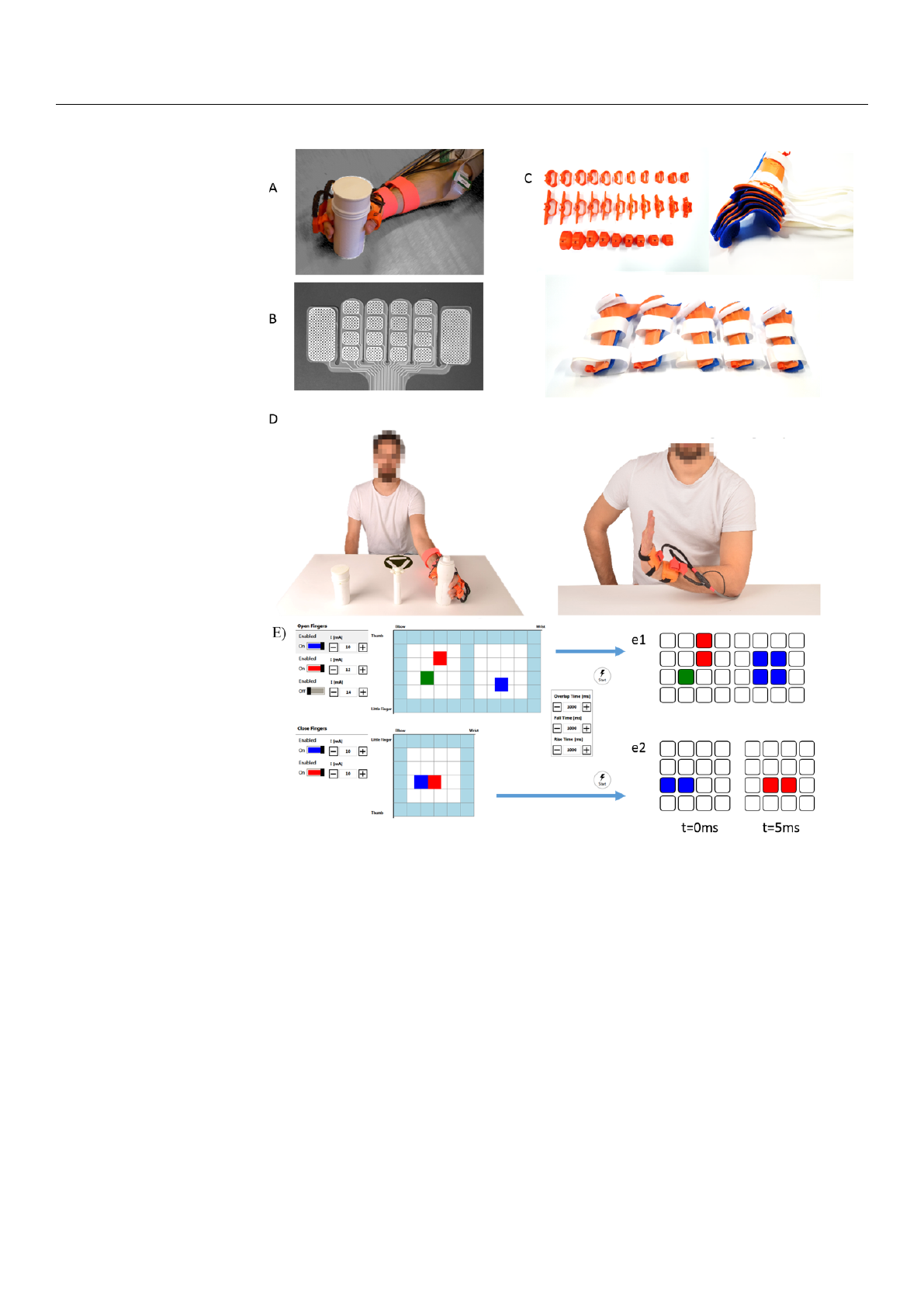
Figure 2.
Wearable NMES system. The wearable system consists of units aimed at providing NMES,
at constraining hand and wrist, and at sensing environmental interaction. Panel (
A
) The orthosis
constrains the dorsal aspect of hand and wrist, and hosts the RF antenna between thumb and index
to improve reliability and repeatability of object detection. A soft ring constrains the thumb in
opposition and includes a force sensor for assessing localised contact force. Panel (
B
) Electrode
arrays used for the trials. Panel (
C
) Anthropometric variability is accounted for by design. The rigid
wrist-constraining orthoses are designed in five sizes and, if warmed, can be adapted to patient-
specific ergonomic needs. Rings, proximal clasp, and distal clasps are soft and produced with a larger
variability. Panel (
D
) Visual and auditory cues in the GUI precede the desired exercise execution.
Panel (
E
) Stimulation maps are defined by virtual electrodes location and intensity of stimulation.
Virtual Electrodes(VEs) can be enabled alone or combined, to fine tune the desired motor response.
e1: frame-wise distribution of the VEs as configured in the GUI for extrinsic extensors; e2: in-frame
patterning for the displayed configuration of extrinsic flexors.
2.2.3. NMES Controller
A GUI, hosted by the CI, represents sets of VEs associated with task-specific stimu-
lation maps. Single VEs and complete stimulation maps can be personalised and tested
in calibration mode. Location and intensity of stimulation to each VE is set on a touch
Loading more pages...