
Supporting Remote Therapeutic Interventions with Mobile Processes
Marc Schickler, R¨
udiger Pryss, Johannes Schobel, Manfred Reichert
Institute of Databases and Information Systems, Ulm University, Germany
{marc.schickler, ruediger.pryss, johannes.schobel, manfred.reichert}@uni-ulm.de
Abstract—Many studies have revealed that homework (e.g.,
relaxation exercises) are crucial for remote therapeutic inter-
ventions. In this context, to monitor whether patients actually
perform their homework and to check whether they perform
it in the right way constitute complex tasks. So far, therapeutic
interventions have not been properly supported by IT systems
and, hence, the opportunities provided by mobile assistance
have been neglected. For example, a smart mobile device may
notify a patient about an assigned homework or motivate him
to accomplish it in time. Moreover, the patient might be further
assisted through a video providing detailed instructions. In
turn, the smart mobile device could inform the therapist of
the homework outcome. In practice, a proper support of the
various types of homework is challenging, even when using
modern IT systems. To remedy this drawback, we propose an
approach integrating mobile services with process management
technology in order to enable the complex coordination tasks
that become necessary in connection with homework. For
example, a process might enable remote monitoring of home-
work, giving therapists the opportunity of timely adjustments.
In addition, the approach allows involving researchers by
providing them with valuable data (e.g., heart rate) gathered
during and after homework. This paper presents an approach
for creating processes that run on smart mobile devices and
enable flexible remote therapeutic intervention support. Such
mobile approach significantly enhances therapy assistance on
one hand and mobile homework-related scenarios on the other.
Keywords-Mobile service, therapeutic intervention, mobile
context, mobile process, mobile assistance, mobile therapy
I. INTRODUCTION
According to numerous clinical studies, therapeutic in-
terventions constitute a fundamental part of most therapies
to increase their efficacy [1], [2]. The variety of therapeutic
interventions, in turn, ranges from simple medication intakes
up to complex homework, which are assigned by a therapist
to the patient. Taking the diversity of useful homework
into account, therapists crave for a proper IT support. In
line with this trend, recent studies (e.g., [3]) revealed that
the use of smart mobile devices is particularly demanded
by therapists [4]. Unfortunately, existing mobile approaches
still show drawbacks. First, they mostly provide specifically
tailored mobile applications and, hence, do not deal with the
diversity of therapeutic interventions. Second, they focus on
the therapist-patient relationship, neglecting other promising
opportunities. Third, features provided by current smart
mobile devices (e.g., sensors) have not been broadly used
for therapeutic interventions yet.
Figure 1: Pursued Objectives
Considering these drawbacks, Fig. 1 illustrates three
fundamental objectives relevant for a proper therapeutic
intervention support. First of all, in addition to smartphones
and tablets, emerging technologies like smartwatches need
to be integrated to address current demands of mobile users.
Second, the opportunities provided by smart mobile device
sensors should be utilized as well. Third, the therapist-
patient relationship needs to be extended to a therapist-
patient-researcher relationship to take benefit from the valu-
able data collected with the smart mobile devices over time.
If these objectives are met, the following advantages will
result:
1) Patients will obtain better treatment as therapeutic
interventions may be personalized, i.e., adjusted to the
specific situation of the patient at hand.
2) Therapists are enabled to provide an optimized and
more efficient treatment as they can monitor and

dynamically adjust therapeutic interventions remotely.
Respective adjustments, for example, might foster
innovative billing models.
3) In the longer term, patients might benefit from new
therapies developed on the basis of the data collected.
4) Therapists can use emerging therapies discovered by
researchers based on the data gathered over time.
5) Researchers discover new therapies or gain new in-
sights into diseases based on the data provided by
patients (e.g., sensor data) as well as by therapists
(e.g., context-based therapy results).
As illustrated, the IT support of therapeutic interventions
is complex. In particular, all (remote) issues not taking place
in the scope of personal meetings (e.g., homework) between
therapist and patients are technically challenging. On the
other, these remote issues require a tight integration with
issues (e.g., general treatment adaptations) that occur during
the personal meetings. Consequently, a holistic view on the
entire procedure is crucial. From a technical perspective,
an overall protocol must be developed to coordinate all
required issues. In the given context, the development of
such a protocol is particularly challenging as both stationary
as well as mobile systems must be considered. Therefore,
we advocate an approach based on mobile processes to
enable the required coordination protocol. If the latter can
be established, the efficacy of therapeutic interventions may
be increased since an effective monitoring of the afore-
mentioned remote issues becomes possible. Based on the
resulting monitoring data, for example, required adaptations
to the therapeutic intervention procedure can be realized in
real time as well as in a more patient-centric manner.
To realize this protocol, first of all, we defined a meta-
model taking the complex organization of therapeutic in-
terventions into account. Based on the meta-model, we
developed a technical solution executing processes on smart
mobile devices. These mobile processes enable us to perform
complex therapeutic interventions for patients assisted by
their smart mobile devices.
This paper shows how mobile processes are realized and
in what way they effectively support therapeutic interven-
tions. In detail, fundamental requirements on one hand,
and the meta-model, main concept, and proof-of-concept
prototype are presented on the other. The remainder of the
paper is structured as follows: Section II discusses elicitated
requirements. Section III presents the meta-model derived
from these requirements. In Section IV, the support of
mobile processes is discussed, whereas Section V deals with
relevant sub-process patterns in more detail. Section VII
gives insights into the proof-of-concept prototype. Finally,
Section VIII discusses related work and Section IX con-
cludes the paper with a summary and outlook.
II. REQUIREMENTS
First of all, we summarize how therapeutic interventions
are traditionally accomplished (i.e., without IT support): The
therapy starts with a first personal meeting of the therapist
and the patient. During this meeting as well as in follow-up
sessions, the therapist creates a comprehensive anamnesis for
the case conceptualization, upon which the remote therapeu-
tic interventions (e.g., homework) are planned. Based on the
anamnesis, the therapist compiles a therapy plan, consisting
of (1) therapeutic interventions, (2) personal appointments
with the patient, and (3) the duration required to achieve
a positive therapy effect for the patient. Concerning the
therapeutic interventions, two intervention types need to be
created by therapists, the one applied during the personal
meetings and the one performed by the patients at home
between the meetings with the therapist. As one of the most
crucial drawbacks of this traditional procedure, homework
cannot be remotely monitored and, hence, therapists are
unable to timely adjust ongoing homework. Additionally,
the exchange of feedback between therapist and patients is
not efficiently supported. As the mobile processes we target
at must cover the variety of therapeutic interventions, pro-
found insights into real-world scenarios are indispensable.
In general, respective insights should be gathered in the
context of large-scale case studies over longer period of
times to better understand actual requirements. Ourselves,
we base the development of the mobile process support
on the experiences we gathered when realizing complex
mobile applications that support therapeutic interventions in
the large scale [5]–[7].
In these case studies, therapists were provided with
specifically tailored mobile applications. Thereby, all studies
revealed that, when using mobile applications, therapeutic
interventions can be supported more efficiently [6]. Regard-
ing the case study in a psychosomatic in-patient clinic, for
example, we learned that the support of homework with
a mobile application is considered as useful in almost all
patient cases [6]. According to a particular feature demanded
in this context, patients shall be notified on their smart
mobile devices about the need to perform their homework.
The latter, in turn, shall be scheduled by a therapist to allow
for a better therapy effect. Table I summarizes the elaborated
requirements that need to be met by mobile processes in
order to efficiently support therapeutic interventions. We
divide the requirements into three categories. (1) Require-
ments related to homework. For example, therapists should
be able to assign media elements to homework, which are
then presented to the patient on his smart mobile device. (2)
Requirements related to the context of a homework. This
context enables us to cope with the demands of therapists on
one hand (e.g., performance of a homework after getting up)
and enables researchers to gather context-sensitive data on
the other. (3) Requirements related to smart mobile devices.
No Title Description
Category I: Homework
1Notification Create notification schema for homework
2Configuration Configure homework (e.g., context, and sensors)
3Versioning Create and manage homework versions
4Feedback Configure feedback schema for homework
5Reuse Use homework for different scenarios
6Media Use media elements for homework (e.g., videos)
Category II: Context
7Notification Bind notification schema to context
8Notification Provide advanced notifications
9Configuration Configure context (e.g., location, etc.)
10 Versioning Create and manage context versions
Category III: Smart Mobile Device
11 Notification Apply notification schema
12 ACR Evaluate context
13 Sensing Use smart mobile device sensors
14 Media Provide media elements
ACR = Automatic Context Recognition
Table I: Elicitated Requirements
For example, the smart mobile device shall provide media
elements to assist patients in performing their homework.
Altogether, 14 fundamental requirements were elicitated.
III. META-MODEL
First of all, the definition of the meta-model needs to
incorporate the lessons learned from the real-world projects.
Second, it needs to capture the complexity of therapeutic
interventions consisting of comprehensive homework, e.g.,
daily back exercises. Homework, in turn, comprise several
activities. For example, the following activities may have to
be performed in the context of a daily back exercise: warm
up, strengthening, and cool down. Therefore, the meta-model
considers homework as well as activities as core entity types.
Furthermore, the meta-model considers the context (e.g.,
being in the living room), in which the homework shall be
performed as well as it takes the sensors (e.g., heart rate) of
smart mobile devices into account.
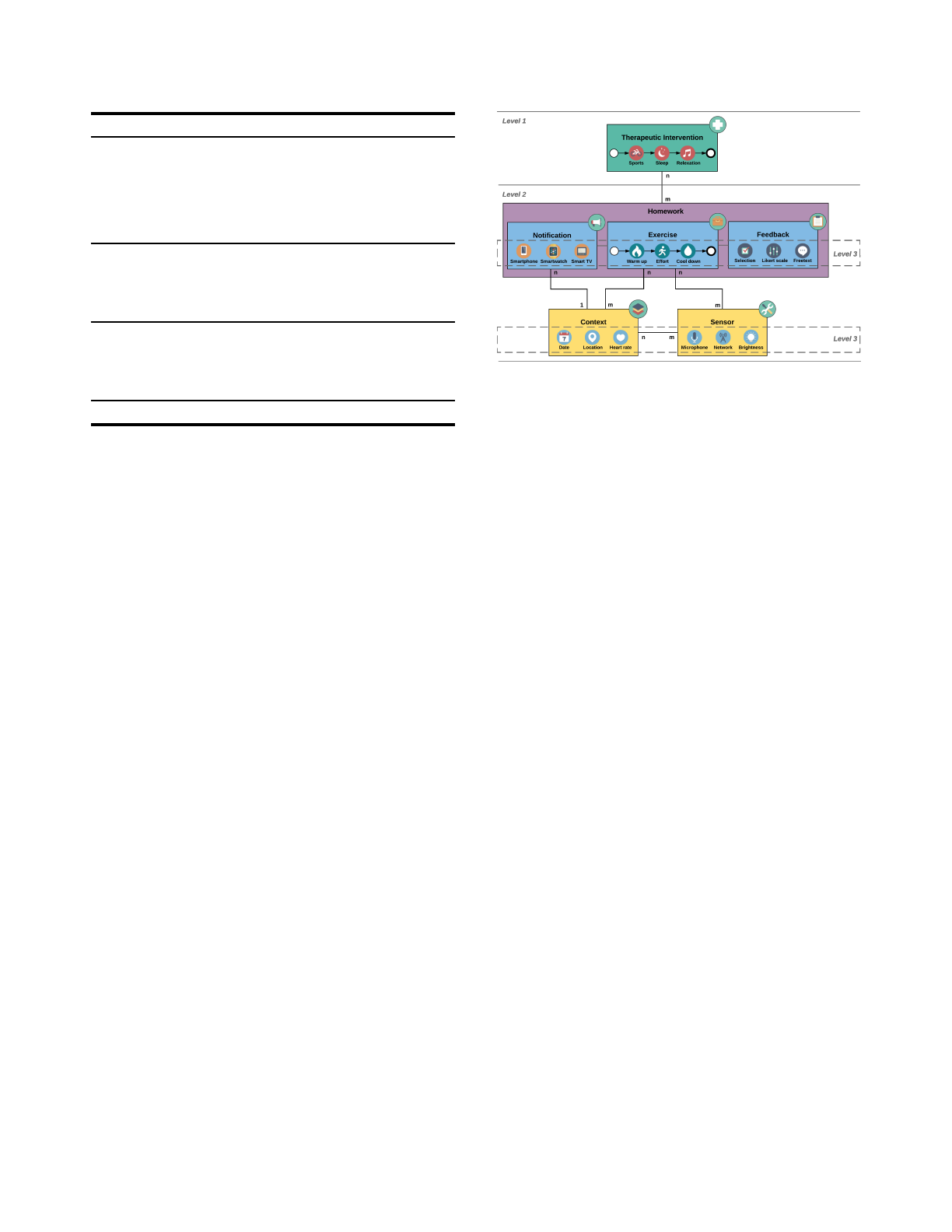
Accordingly, the meta-model is built up on three levels (cf.
Fig. 2). On the first level, a Therapeutic Intervention consists
of 1up to n Homework, for which an execution order needs
to be defined. On the second level, a particular Homework
encompasses a Notification, an Exercise, and a Feedback. In
addition, the meta-model considers a Context and a Sensor
on the second level. Sensor covers, for example, the sensors
of smart mobile devices gathering data during an exercise
(e.g., heart rate). While a Sensor is related to an Exercise
and a Context, a Context may be related to a Notification
and an Exercise. On the third level, the highlighted entities
encompass activities, which either need to be performed by
a patient (e.g., a warm up activity after getting up) or be
automated (e.g., sensing the heart rate during a warm up),
i.e., run on smart mobile device of a patient.
Figure 2: Meta-Model
IV. MOBILE PROCESS
This section introduces the mobile processes developed
on the basis of the meta-model. Fig. 3 shows a therapeutic
intervention represented in terms of a mobile process. To be
more precise, the mobile process consists of three process
fragments. Each fragment, in turn, corresponds to a particu-
lar homework, whose execution order is determined by the
mobile process. Homework, in turn, always encompasses
three mobile process activities, i.e., a notification activity,
an exercise activity, and a feedback activity. These activities,
in turn, are always executed in the order Notification →
Exercise →F eedback. That means, a patient is notified
that an exercise needs to be accomplished. In turn, the
patient shall provide feedback to the therapist. In practice,
each activity is executed on a smart mobile device. Finally,
homework are always executed in a particular context.
For example, a homework might have to be performed in
the living room after getting up. Note that the concrete
implementation of all activities representing homework and
being executed on the smart mobile device depends on the
concrete homework scenario on one hand and on the used
mobile platform on the other.
The analysis of the real-world scenarios revealed that
activities representing exercises require a further itemization
(cf. Fig. 4, Exercise level). To be more precise, therapists
want to create exercises composed on several activities.
For example, an exercise may comprise a warm-up activity,
a push-up activity, and a cool-down activity. In addition,
therapists may want to use the sensors of smart mobile
devices to collect patient data during these activities. We
therefore integrated a context-based sensing activity with
exercises. Note that our practical insights revealed that both
the notification and the feedback activity must be itemized in
the same way as the exercise activity. Since the notification
and feedback activities are similar to the exercise activity,
we omit a more detailed discussion.
Practical insights further showed that exercise activities
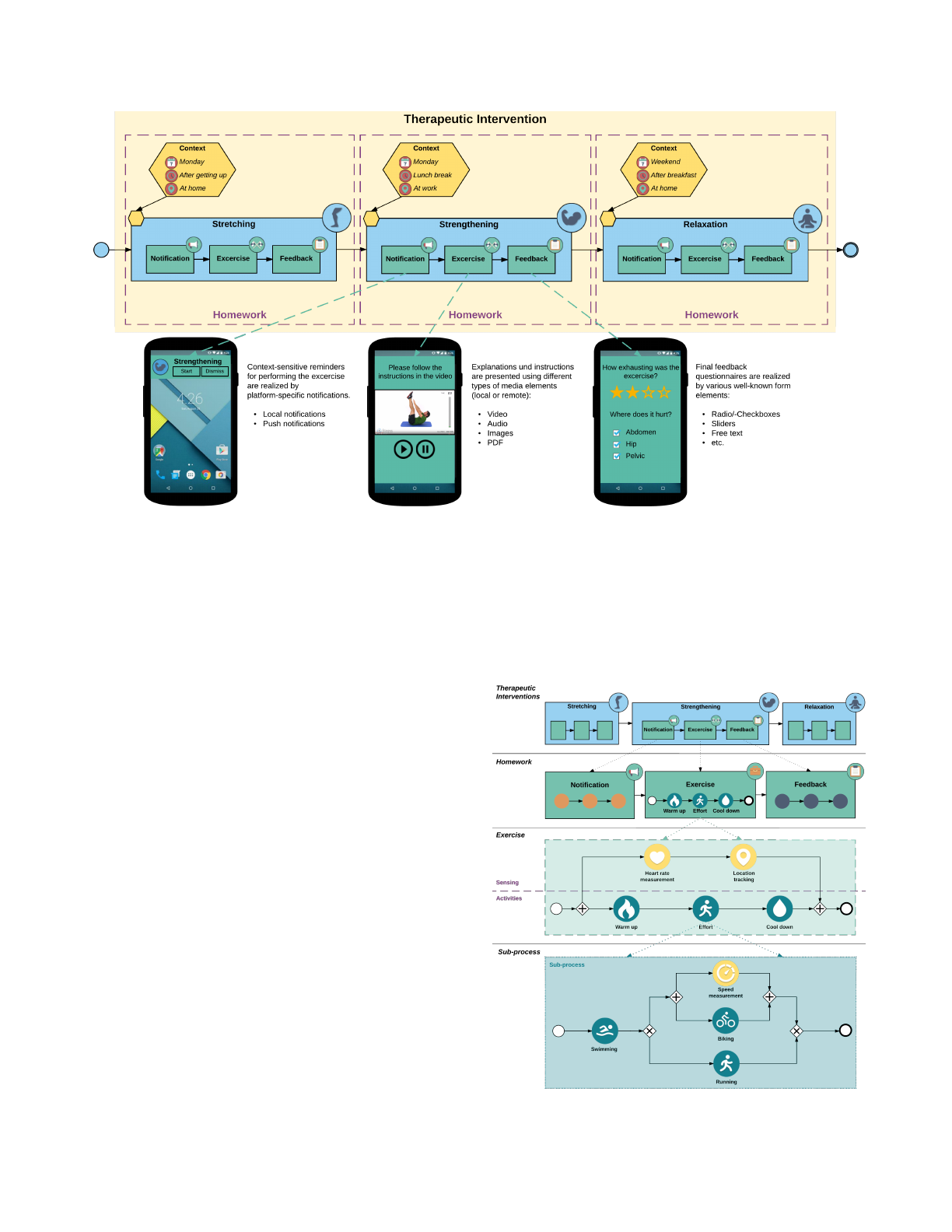
Figure 3: Remote Therapeutic Intervention with three Homework Fragments
require a more flexible concept to meet the requirements
of therapists. Therefore, we allow for the implementation
of exercise activities as sub-processes. For example, activity
effort may be implemented as a sub-process (cf. Fig. 4, Sub-
process level), containing activity swimming, followed by a
decision that evaluates whether swimming shall be followed
by activity biking or activity running. If activity biking is
chosen, the biking speed will be measured by a context-
based sensing activity. Note that the contextual information,
required to evaluate whether biking or running shall be
chosen, needs to be specified by therapists.
Fig. 4 illustrates the described exercise itemization as
well as the possible use of sub-processes. Furthermore,
it is shown that the mobile processes are organized in
five different levels. These levels constitute the basis for
the modeling component that enables therapists to create
therapeutic interventions themselves. More precisely, the
modeling component offers features that consider the differ-
ent levels in order to guide the therapists during the creation
of therapeutic interventions in terms of mobile processes.
Regarding guidance, therapists are restricted to only use
elements that are allowed for a specific level. In particular,
on the exercise level, our modeling component provides
various activity templates. The latter cover frequent sce-
narios occurring in the context of exercises. For example,
the modeling component provides activity templates for
measuring the heart rate or filling in a questionnaire. Note
that therapists may create exercises solely based on the
available activity templates. In practice, however, there exist
scenarios in which the provided activity templates are not
sufficient. For example, therapists may request an activity
template for measuring skin conductance, while filling in
a questionnaire in parallel. In such a case, the application
Figure 4: Mobile Process
developer needs to implement the missing activity template.
After releasing the newly implemented activity template, it
may be used by therapists when modeling the exercise.
Therapeutic interventions created with the modeling com-
ponent are transformed into executable processes running
on smart mobile devices. The corresponding transformation
procedure ensures that the resulting mobile processes can be
correctly executed by a mobile process engine (e.g., the one
we presented in [8]). Finally, the mobile process is deployed
to the mobile application, which relies on the mobile process
engine for executing the mobile processes.
V. SUB-PROCESS PATTERNS
If therapists request new activity templates for defining
concrete therapeutic interventions, these templates must be
realized by an application developer. In several case studies,
we learned that the development of new activity templates
is (1) easily possible and (2) can be mostly accomplished
without involving therapists [9]. Regarding the use of sub-
processes, we further learned that requests from therapists
frequently require the involvement of application developers,
causing challenging debates between application developers
and therapists. For example, two activities may have to
be executed concurrently. However, contemporary mobile
process engines do not provide such concurrency support.
For this purpose, a specifically implemented sub-process is
required, which can then be executed by the mobile process
engine.
Regarding the support of application developers, we iden-
tified four fundamental patterns, which significantly ease the
handling of sub-processes for them. We introduce these sub-
process patterns in the following and discuss how they are
evaluated during the development.
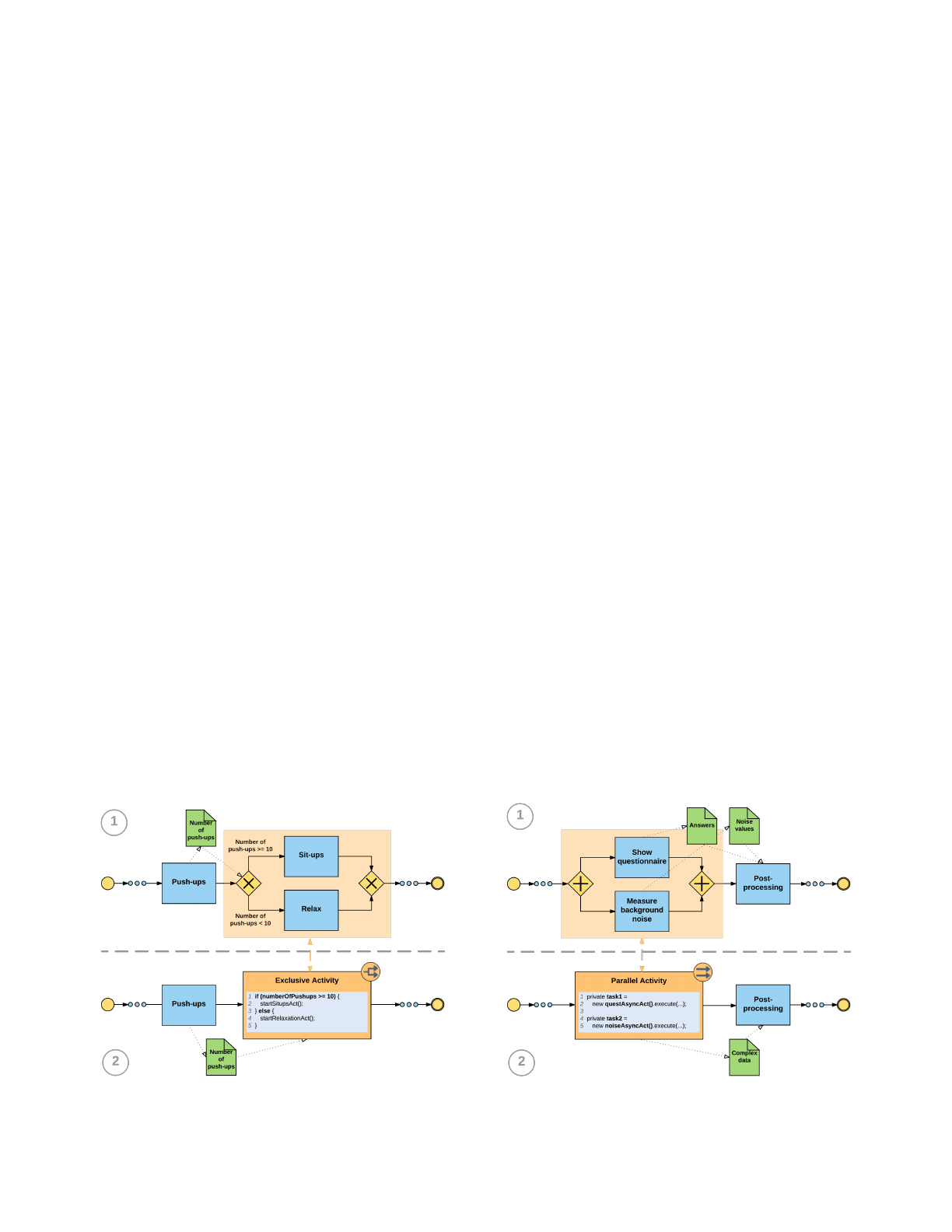
Figure 5: Decision Pattern
A. Decision Pattern
Fig. 5 1
shows a sub-process pattern, called Decision
Pattern, in which two activities may be chosen alternatively
(i.e., exclusive decision); i.e., during run time exactly one
of the two activities may be executed. The decision, which
activity will be actually chosen, is based on data that is
(1) produced by a preceding activity or (2) provided by
the therapist. In Fig. 5 1
, for example, depending on the
number of performed push-ups and determined by the push-
ups, the mobile process engine decides at run time whether
the patient shall perform sit-ups or relax.
When a decision as shown in Fig. 5 1
is required by a
therapist, an application developer must particularly evaluate
if one (e.g., sit-ups in Fig. 5 1
) or more activity templates
not exist. In the latter case, the application developer must
decide whether to provide the missing activity templates or
to replace the entire Decision Pattern with a new activity
template instead of the pattern. To be more precise, an
application developer is supported in deciding whether he
applies the Decision Pattern or uses a specifically imple-
mented activity template. For example, if complex forms
are required for missing activity templates of the Decision
Pattern, in most cases, a new activity template replacing the
entire Decision Pattern fits practical demands best.
B. Parallel Pattern I
The approach of replacing a pattern by a specifically
implemented activity template (cf. Fig. 6 2
) is applied in
the context of the Parallel Pattern I as well (cf. Fig.
6). However, there is another case to be considered by
application developers. In certain situations, it needs to be
evaluated, whether or not the activities shall be executed
concurrently. As existing mobile process engines [9] do not
allow for a concurrent execution, a specifically implemented
Figure 6: Parallel Pattern I
Loading more pages...